 E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 17(1); 2024 > Article
-
Original Article
Caregiver Burden of Patients With Huntington’s Disease in South Korea -
Chan Young Lee1*
 , Chaewon Shin2*, Yun Su Hwang3,4, Eungseok Oh5, Manho Kim6, Hyun Sook Kim7, Sun Ju Chung8, Young Hee Sung9, Won Tae Yoon10, Jin Whan Cho11, Jae-Hyeok Lee12, Han-Joon Kim6, Hee Jin Chang6, Beomseok Jeon6, Kyung Ah Woo6, Seong-Beom Koh13, Kyum-Yil Kwon14, Jangsup Moon6,15, Young Eun Kim16, Jee-Young Lee17
, Chaewon Shin2*, Yun Su Hwang3,4, Eungseok Oh5, Manho Kim6, Hyun Sook Kim7, Sun Ju Chung8, Young Hee Sung9, Won Tae Yoon10, Jin Whan Cho11, Jae-Hyeok Lee12, Han-Joon Kim6, Hee Jin Chang6, Beomseok Jeon6, Kyung Ah Woo6, Seong-Beom Koh13, Kyum-Yil Kwon14, Jangsup Moon6,15, Young Eun Kim16, Jee-Young Lee17
-
Journal of Movement Disorders 2024;17(1):30-37.
DOI: https://doi.org/10.14802/jmd.23134
Published online: September 11, 2023
1Department of Neurology, Ewha Womans University Mokdong Hospital, Ewha Womans University College of Medicine, Seoul, Korea
2Department of Neurology, Chungnam National University Sejong Hospital, Chungnam National University College of Medicine, Sejong, Korea
3Department of Neurology, Jeonbuk National University Hospital, Jeonbuk National University Medical School, Jeonju, Korea
4Research Institute of Clinical Medicine and Biomedical Research Institute, Jeonbuk National University Hospital, Jeonbuk National University Medical School, Jeonju, Korea
5Department of Neurology, Chungnam National University Hospital, Chungnam National University College of Medicine, Daejeon, Korea
6Department of Neurology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea
7Department of Neurology, Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea
8Department of Neurology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
9Department of Neurology, Gil Medical Center, Gachon University College of Medicine, Incheon, Korea
10Department of Neurology, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea
11Department of Neurology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
12Department of Neurology, Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea
13Department of Neurology, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Korea
14Department of Neurology, Soonchunhyang University Seoul Hospital, Seoul, Korea
15Department of Genomic Medicine, Seoul National University Hospital, Seoul, Korea
16Department of Neurology, Hallym University Sacred Heart Hospital, Anyang, Korea
17Department of Neurology, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea
- Corresponding author: Jee-Young Lee, MD, PhD Department of Neurology, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul National University College of Medicine, 20 Boramae-ro 5-gil, Dongjak-gu, Seoul 07061, Korea / Tel: +82-2-870-2476 / Fax: +82-2-831-2826 / E-mail: wieber04@snu.ac.kr
- *These authors contributed equally to this work.
Copyright © 2024 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,922 Views
- 151 Download
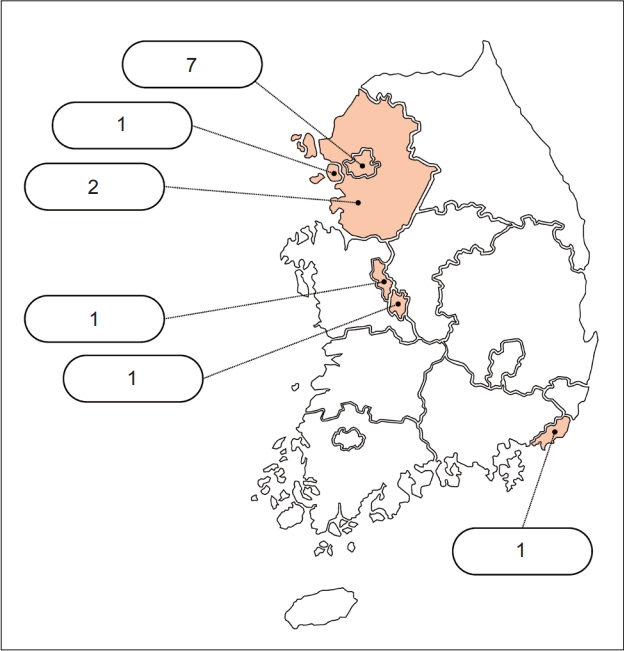
Figure & Data
References
Citations
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite- Figure
-


- Related articles
-
- A Practical Guide for Clinical Approach to Patients With Huntington’s Disease in Korea
- Copper Deficiency Myeloneuropathy in a Patient With Wilson’s Disease
- A Survey of Perspectives on Telemedicine for Patients With Parkinson’s Disease
- The Frequency of Korean Patients With Parkinson’s Disease Carrying GBA Mutations in a Subgroup With Age at Onset ≤ 55 Years Old
- Subjective Cognitive Complaints in Cognitively Normal Patients With Parkinson’s Disease: A Systematic Review

Manho Kim
March 31, 2024