Department of Oral and Maxillofacial Surgery, National Hospital Organization, Kyoto Medical Center, Kyoto, Japan
Corresponding author: Kazuya Yoshida, DDS, PhD Department of Oral and Maxillofacial Surgery, National Hospital Organization, Kyoto Medical Center, 1-1 Mukaihata-cho, Fukakusa, Fushimi-ku, Kyoto 612-8555, Japan / Tel: +81-75-641-9161 / Fax: +81-75-643-4325 / E-mail: omdystonia@gmail.com
• Received: November 28, 2023 • Revised: December 24, 2023 • Accepted: January 13, 2024
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Hemimasticatory spasm (HMS) manifests as unilateral, paroxysmal contractions of the jaw-closing muscles, resulting in brief twitches and/or spasms [1-3]. HMS can be treated with oral medication, botulinum toxin therapy, and microvascular decompression surgery. Although botulinum toxin injection into the affected muscles is believed to be the most effective option [1-3], possible side effects include hemifacial asymmetry due to atrophy of the injected muscle and masticatory disturbance related to a reduction in bite force [4]. Muscle afferent block (MAB) therapy involving the injection of a local anesthetic is effective for relieving muscle pain without reducing muscle strength [5]. The author describes a case in which HMS was treated with MAB and an occlusal splint.
A 51-year-old woman visited a neurologist complaining of involuntary paroxysmal contractions and pain on the left side of her face, numbness on the ulnar side of her left hand, and cramps in her left leg. A neurologist suspected cramps, myoclonus, stiff-person syndrome, and Isaacs syndrome, so she conducted the appropriate examinations. No abnormalities were observed. The neurologist prescribed clonazepam 1 mg daily, which reduced the frequency of the patient’s involuntary movements.
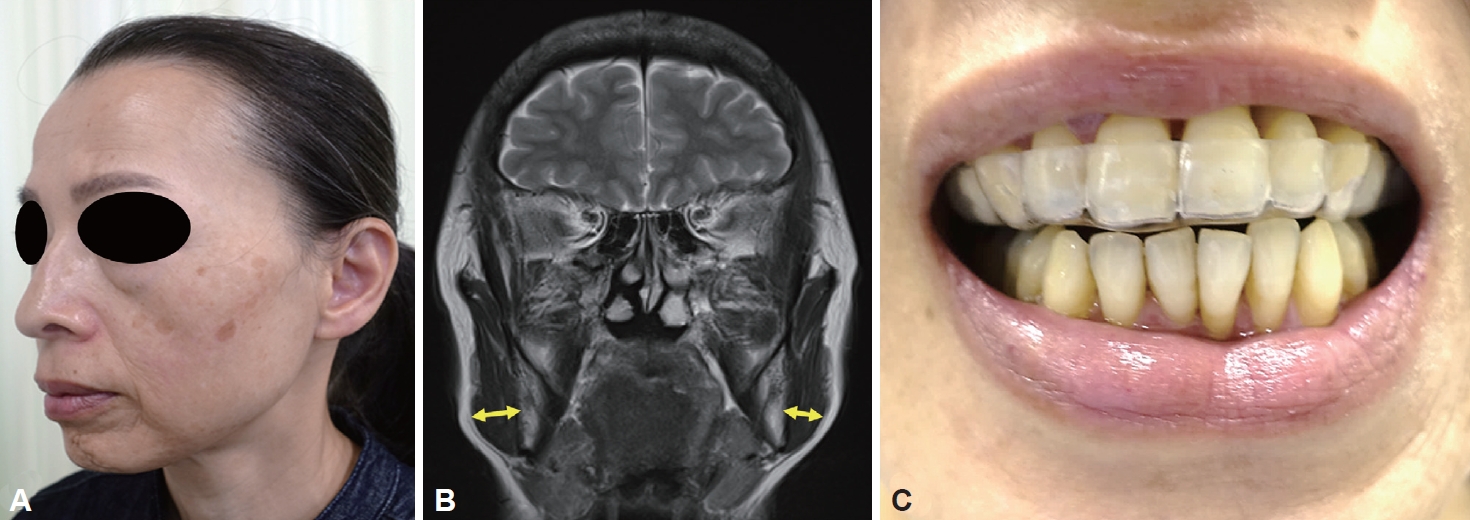
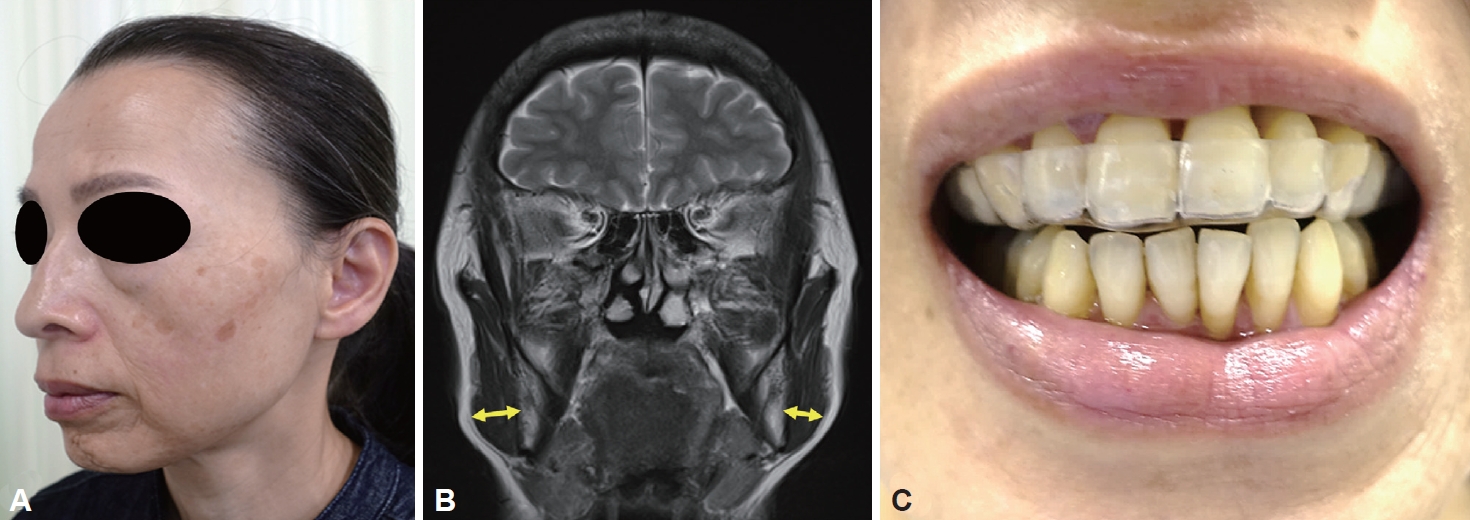
Two months after her first visit to a neurologist, the patient was referred to our department because of pain in the left lower first molar. She also experienced paroxysmal muscle contractions and severe pain on the left side of her face (Supplementary Video 1 in the online-only Data Supplement). The left masseter muscle was slightly atrophied (Figure 1A, B). On the right side, the bite force measured on the bilateral molar regions using an occlusal force meter [4] was 258.7 N. On the left side, the bite force was 48 N, which was considerably lower owing to muscle pain. She also had morphea on the left side of her face (Figure 1A, Supplementary Video 1 in the online-only Data Supplement), both lower limbs, and chest. The patient developed apical periodontitis of the lower left first molar, which was eventually removed.
Electromyography (EMG) of the left masseter muscle showed several irregular brief bursts of multiple motor unit potentials (Supplementary Figure 1A in the online-only Data Supplement). The masseter reflex and silent period were not elicited by tapping the chin with a reflex hammer during prolonged spasms with continuous bursts (Supplementary Figure 1B in the online-only Data Supplement). A dry macaroni was placed between the upper and lower molars, and the patient was asked to crush the macaroni in a single bite [6]. However, no silent periods were detected.
Although botulinum toxin therapy is effective, it can cause left-sided muscle atrophy and hemifacial asymmetry. Furthermore, masticatory disturbances may develop owing to reduced bite force on the affected side. The patient refused botulinum toxin therapy. The author administered MAB therapy via an injection of a local anesthetic [4,5]. Three milliliters of 0.5% lidocaine (Xylocaine; Sandoz K.K., Tokyo, Japan) was injected into the left masseter muscle [4,5]. The injection was repeated once a week for 4 weeks. She had occlusal discomfort, and an occlusal splint was inserted into the maxilla (Figure 1C) with a mild effect [7]. Clonazepam (1 mg daily) was continued. Because HMS persisted during sleep, she wore a splint while sleeping. The number of spasms gradually decreased from 10 times per day to 2–3 times per week, and masseter muscle pain on the left side was relieved, decreasing from 16 to 3 points (total pain score [0–40 points] on the Oromandibular Dystonia Rating Scale) [4]. The bite force on the left side increased from 48 N to 179.5 N. During the 1-year follow-up period, the subjective improvement rate (0% being ineffective and 100% a complete cure) was maintained at 75%.
HMS is a rare unilateral movement disorder caused by dysfunction of the motor trigeminal nerve and is characterized by paroxysmal contractions of the jaw-closing muscles, mainly the masseter and/or temporalis [1-3]. A neurologist may diagnose a patient with HMS with hemifacial spasm or unilateral oromandibular dystonia. Dentists and oral surgeons may diagnose temporomandibular joint disorders or bruxism. Characteristic features such as unilateral painful paroxysmal spasms, scleroderma or morphea, absence of sensory trick and cocontraction, and facial hemiatrophy should be considered for a differential diagnosis. EMG may provide important information about the loss of the silent period and irregular bursts of high-frequency motor units [1-3].
Botulinum toxin therapy is believed to be the most effective treatment option for HMS [1-3]. However, in the present case, mild muscle atrophy and a significant reduction in bite force were observed on the affected side. Botulinum toxin therapy exacerbates atrophy of the muscles of the left side of the face and causes masticatory disturbances due to reduced bite force. MAB blocks muscle afferents for the treatment of focal dystonia, and a local injection of lidocaine reduces the effectiveness of muscle spindle afferents without causing unwanted weakness [4,5]. Previous studies have shown that MAB is significantly more effective than saline injections for oromandibular dystonia [5]. Although additional studies are needed to clarify the mechanism underlying the effects of MAB therapy, local injections of lidocaine can block afferents in the muscle spindle [4,5]. In a previous study [5], the mean response of the jaw-closing muscles (70%) was significantly greater (p < 0.02) than that of the jaw-opening muscles (38%). The significantly greater improvement in the condition of patients after receiving an injection into the jaw-closing muscles instead of an injection into the jaw-opening muscles might be related to more muscle spindles. The masseter muscle has an abundance of muscle spindles; therefore, MAB of the masseter muscle will be useful in the treatment of HMS.
Sensory trick splints have been reported to be effective in patients with oromandibular dystonia who exhibit sensory tricks, especially jaw-closing dystonia [7]. However, no sensory tricks were observed in the patient in this study. Many HMS patients know from experience that forcing the mouth to open during a spasm can suppress the spasm [2]. Opening the mouth may stretch the jaw-closing muscles, affecting the signal from the muscle spindles. A case in which a permanent dental splint slightly relieved HMS symptoms has been reported [2]. Increasing the occlusal vertical dimension with a splint may slightly stretch the closing muscles, decreasing the likelihood of spasm. More studies with larger samples of patients are needed to test this hypothesis.
A rhythmic left masseter muscle twitch was observed in a patient with hemimasticatory spasm. Involuntary contractions can be elicited during chewing and often result in tongue biting.
Supplementary Figure 1.
EMG recordings of left masseter muscle activity via surface electrodes. A: The left masseter muscle demonstrated irregular bursts of multiple motor unit potentials during spasm. B: The left masseter did not show silent periods when the chin was tapped using a reflex hammer during unloading of the bite force during prolonged spasms. EMG, electromyography.
This study was performed in accordance with the tenets of the Declaration of Helsinki after being approved by the Institutional Review Board and Ethics Committee of the Kyoto Medical Center (10-27). Informed consent was obtained from the patient.
Conflicts of Interest
The author has no financial conflicts of interest.
Funding Statement
This study was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (grant number: JP22K10091).
Acknowledgments
None
Figure 1.
Hemimasticatory spasm of the left masseter was observed in a 51-year-old female patient. A: Morphea and slight hemiatrophy were observed on the left side of the face. B: Magnetic resonance imaging revealed that the left masseter was slightly atrophied compared with the right masseter. C: An occlusal splint was inserted into the upper jaw.
REFERENCES
1. Cruccu G, Inghilleri M, Berardelli A, Pauletti G, Casali C, Coratti P, et al. Pathophysiology of hemimasticatory spasm. J Neurol Neurosurg Psychiatry 1994;57:43–50.ArticlePubMedPMC
2. Esteban A, Traba A, Prieto J, Grandas F. Long term follow up of a hemimasticatory spasm. Acta Neurol Scand 2002;105:67–72.ArticlePubMedPDF
3. Ray S, Kamble N, Yadav R, Pal PK. Long-term outcome of hemimasticatory spasm. J Mov Disord 2022;15:146–150.ArticlePubMedPMCPDF
4. Yoshida K. Botulinum toxin therapy for oromandibular dystonia and other movement disorders in the stomatognathic system. Toxins (Basel) 2022;14:282.ArticlePubMedPMC
5. Yoshida K, Kaji R, Kubori T, Kohara N, Iizuka T, Kimura J. Muscle afferent block for the treatment of oromandibular dystonia. Mov Disord 1998;13:699–705.ArticlePubMed
6. Yoshida K. Masticatory muscle responses associated with unloading of biting force during food crushing. J Oral Rehabil 1998;25:830–837.PubMed
7. Yoshida K. Sensory trick splint as a multimodal therapy for oromandibular dystonia. J Prosthodont Res 2018;62:239–244.ArticlePubMed
Figure & Data
References
Citations
Citations to this article as recorded by
Hemimasticatory spasm: a series of 17 cases and a comprehensive review of the literature Kazuya Yoshida Frontiers in Neurology.2024;[Epub] CrossRef
 E-submission
E-submission




 PubReader
PubReader ePub Link
ePub Link Cite
Cite