Department of Neurology, National Cerebral and Cardiovascular Center, Suita, Japan
Corresponding author: Takeshi Yoshimoto, MD, PhD Department of Neurology, National Cerebral and Cardiovascular Center, 6-1 Kishibe-Shimmachi, Suita, Osaka 564-8565, Japan / Tel: +81-6-6170-1070 / Fax: +81-6-6170-1348 / E-mail: yoshimototakeshi1982@ncvc.go.jp
• Received: February 13, 2023 • Revised: March 11, 2023 • Accepted: March 17, 2023
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Micrographia is a neurological syndrome that causes a subject’s handwritten letters to become abnormally small as a result of smaller-than-normal letter strokes [1]. The leading causes of micrographia are Parkinson’s disease (PD), progressive supranuclear palsy, Huntington’s disease, and corticobasal degeneration; other Parkinson’s syndromes are not implicated [1]. Micrographia can also be caused by cerebral infarction and intracerebral hemorrhage, albeit rarely; the lesions are mainly located in the left hemisphere, including the basal ganglia, and the left hemisphere plays a dominant role in language processing [1]. There are two types of micrographia. The first type is characterized by a gradual decrease in letter size as writing progresses, and the second type is characterized by an abnormally small letter size from the beginning. Regarding the type of micrographia that is characterized by a gradual decrease in letter size, one study reported that the basal ganglia were not involved and that levodopa was ineffective [2]. Dopamine transporter single-photon emission computed tomography (DAT-SPECT) is an established imaging modality for identifying diseases involving presynaptic dopaminergic abnormalities [3]; therefore, DAT-SPECT may play a key role in determining whether micrographia is associated with nondopaminergic pathways. We describe a patient with micrographia due to cerebral infarction who underwent DAT-SPECT to investigate dopamine transporter dynamics.
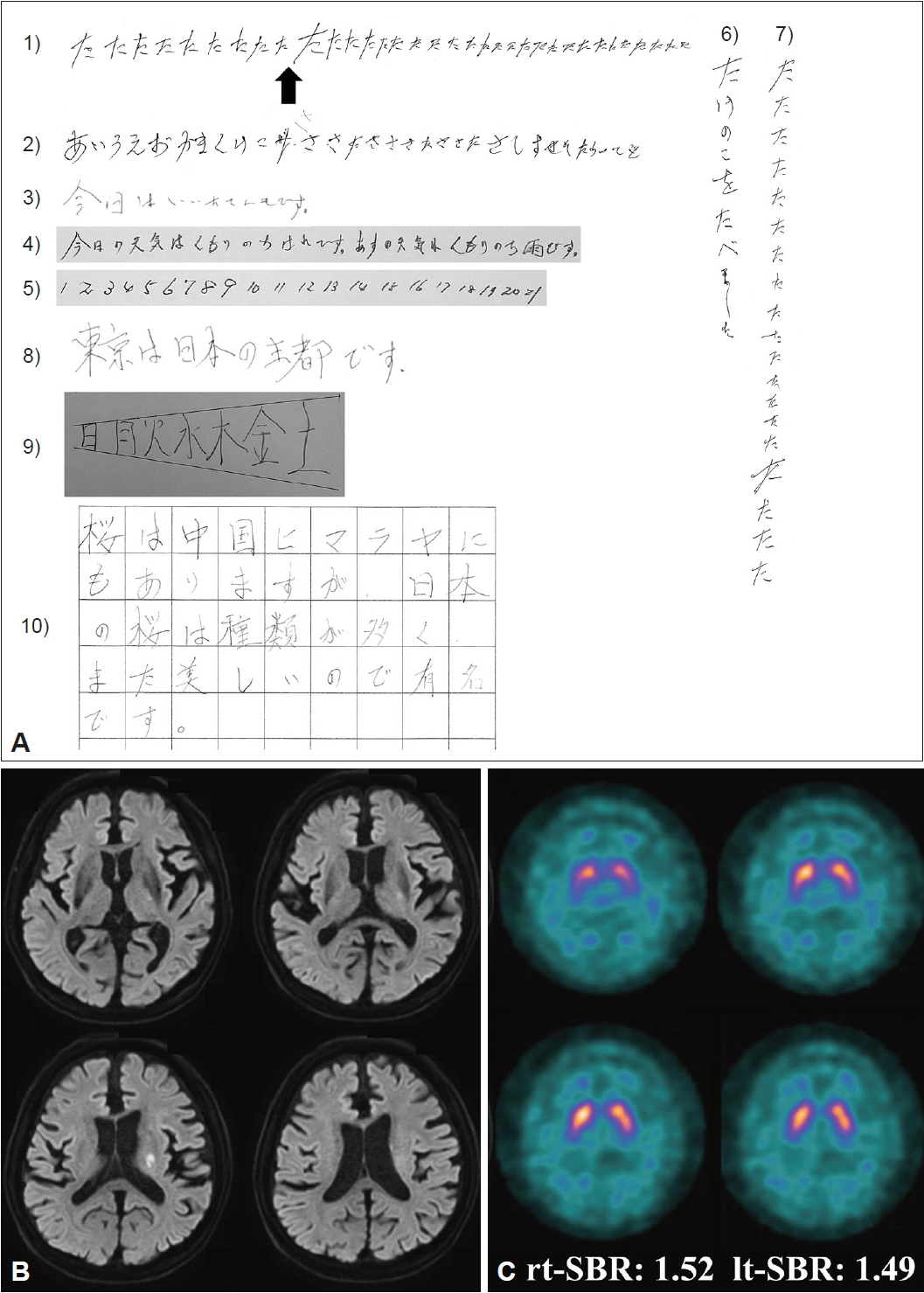
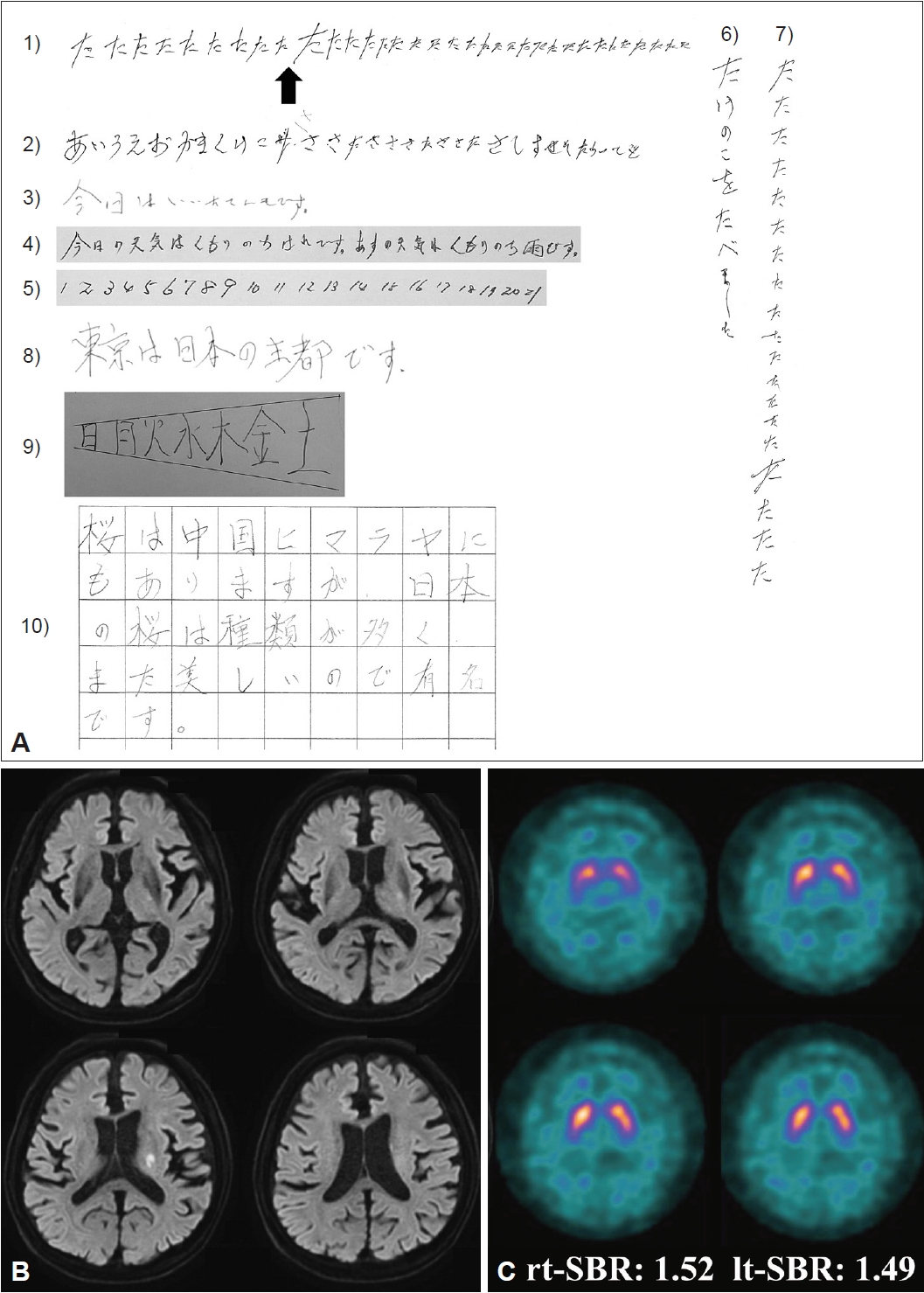
A 79-year-old man experienced mild difficulty in writing things down (Day 0) and visited our hospital on Day 10. His blood pressure was 122/88 mmHg, and his pulse rate was 75 beats/minute with a regular rhythm. Neurological examination revealed dysarthria, mild right-sided hemiparalysis, and micrographia but no parkinsonism or apraxia. His handwritten letters became progressively smaller over the course of a single sentence. His micrographia was observed in both vertical and horizontal writing (Figure 1A, Supplementary Video 1 in the online-only Data Supplement). However, micrographia was not observed when he wrote slowly or when visual cues were provided (Figure 1A). Baseline diffusion-weighted magnetic resonance imaging on Day 10 revealed abnormal hyperintensity in the left corona radiata and left posterior limb of the internal capsule (Figure 1B), and magnetic resonance angiography revealed no steno-occlusion of the intracranial arteries. DAT-SPECT showed that the striatal-specific binding ratio was 1.52 on the right side and 1.49 on the left side, with no decreased uptake in the bilateral striatum on Day 15 (Figure 1C). Follow-up magnetic resonance imaging revealed recurrent asymptomatic acute cerebral infarcts in multiple regions on Day 18. A diagnosis of cardioembolic stroke was made because a transthoracic echocardiogram revealed left ventricular hypokinesis due to a previous myocardial infarction; as a result, warfarin was initiated. His mild right-sided hemiparalysis and micrographia had improved slightly when he was discharged from the hospital.
In this case, micrographia was caused by cerebral infarction in the left corona radiata and left posterior limb of the internal capsule, although DAT-SPECT showed preservation of striatal uptake. This is the first report in which DAT-SPECT radiologically suggested that micrographia with a gradual decrease in letter size due to cerebral infarction may not be associated with presynaptic dopaminergic dysfunction. The left-sided striatal uptake appeared to be slightly lower than the right-sided uptake in this case. However, a healthy population without PD may also have a slight laterality of the specific binding ratio on DAT-SPECT because when the absolute values of the laterality of the specific binding ratio were calculated by subtracting the specific binding ratio value of one side from that of the contralateral side, the median value of the laterality of the specific binding ratio in healthy subjects was 0.29 (interquartile range 0.16– 0.48) [4]. The laterality of striatal uptake on DAT-SPECT in our case may be within normal limits.
In a functional magnetic resonance imaging study on PD, micrographia with a gradual decrease in letter size was shown to be related to dysfunction of the left basal ganglia motor circuit and connectivity between the left rostral supplementary motor area and rostral cingulate motor area, while micrographia with a small letter size from the beginning was related to dysfunction of only the left basal ganglia motor circuit [2]. In our patient, lesions were observed in the left corona radiata and left posterior limb of the internal capsule, suggesting that disrupted connectivity between the left rostral supplemental motor cortex and posterior putamen was responsible for micrographia with a gradual decrease in letter size.
We hypothesize that there is no presynaptic dopaminergic deficiency in this case of micrographia with a gradual decrease in letter size. In one report, DAT-SPECT findings did not correlate with micrographia in PD [5]. In addition, levodopa had a positive effect on micrographia characterized by an initial small letter size but no effect on micrographia characterized by a gradual decrease in letter size over the course of writing [2]. In a case report of micrographia with an initial small letter size due to cerebral infarction, DAT-SPECT revealed decreased striatal uptake [6], whereas in our case of micrographia with a gradual decrease in letter size, striatal uptake was preserved. Therefore, micrographia characterized by a gradual decrease in letter size cannot be attributed to presynaptic dopaminergic deficiency.
Repetition of the Japanese character “ta”. The letter size progressively decreased, increased after a break, but then gradually decreased again.
Notes
Ethics Statement
All procedures performed for this case report were in accordance with the ethical standards of the National Cerebral and Cardiovascular Center research committee and with the CARE guidelines. Patient consent was obtained by written documentation.
Conflicts of Interest
The authors have no financial conflicts of interest.
Handwriting samples for the patient, magnetic resonance imaging and DAT-SPECT images. A: Handwriting showing micrographia. 1) Repetition of the Japanese character “ta” in horizontal writing. The letter size progressively decreased, recovered after a break (black arrow), but then gradually decreased again. 2) Repetition of various Japanese characters in horizontal writing. The letters progressively decreased in size. 3) Horizontal writing of the sentence “It’s sunny today.” The letters progressively decreased in size. 4) Horizontal writing of the sentence “It was cloudy and then sunny today. It will be cloudy and then rainy tomorrow.” The letter size progressively decreased. 5) Repeated numbers in horizontal writing; the characters progressively decreased in size. 6) Vertical writing of the sentence “I ate a bamboo shoot.” The letters progressively decreased in size. 7) Repetition of the Japanese character “ta”. The letter size progressively decreased, recovered after a break, but then gradually decreased again. 8) The sample sentence with no micrographia was written slowly and translates to “Tokyo is the capital of Japan.” The letter size was constant throughout. The first of the two characters, which translates to “capital”, was incorrectly written in Japanese. 9) A sample of consecutive weekdays (Sunday, Monday, Tuesday, Wednesday, Thursday, Friday, and Saturday) written in Japanese with no micrographia. Visual cues were presented, prompting the patients to progressively increase the size of the characters; the letter size gradually increased. 10) Sentence in which each character was written within a grid square. The sentence translates to “Cherry blossoms bloom in the Himalayas, extending to China; moreover, Japanese cherry blossoms are famous for their variety and beauty.” The letter size remained constant. B: Diffusion-weighted magnetic resonance imaging of the brain on Day 10 revealed abnormal hyperintensity in the left corona radiata and left posterior capsule of the internal capsule. C: DAT-SPECT showed that the right-side striatal specific binding ratio was 1.52 and the left-side was 1.49. DAT-SPECT revealed normal uptake in the bilateral striatum. DAT-SPECT, dopamine transporter single-photon emission computed tomography; rt-SBR, right-side striatal specific binding ratio; lt-SBR, left-side striatal specific binding ratio.
REFERENCES
1. Inzelberg R, Plotnik M, Harpaz NK, Flash T. Micrographia, much beyond the writer’s hand. Parkinsonism Relat Disord 2016;26:1–9.ArticlePubMed
2. Wu T, Zhang J, Hallett M, Feng T, Hou Y, Chan P. Neural correlates underlying micrographia in Parkinson’s disease. Brain 2016;139(Pt 1):144–160.ArticlePubMedPMC
3. Ma KKY, Lin S, Mok VCT. Neuroimaging in vascular parkinsonism. Curr Neurol Neurosci Rep 2019;19:102.ArticlePubMedPMCPDF
4. Shigekiyo T, Arawaka S. Laterality of specific binding ratios on DAT-SPECT for differential diagnosis of degenerative parkinsonian syndromes. Sci Rep 2020;10:15761.ArticlePubMedPMCPDF
5. Eklund M, Nuuttila S, Joutsa J, Jaakkola E, Mäkinen E, Honkanen EA, et al. Diagnostic value of micrographia in Parkinson’s disease: a study with [123I]FP-CIT SPECT. J Neural Transm (Vienna) 2022;129:895–904.ArticlePubMedPMCPDF
6. Kim JS, Im JH, Kwon SU, Kang JH, Lee MC. Micrographia after thalamo-mesencephalic infarction: evidence of striatal dopaminergic hypofunction. Neurology 1998;51:625–627.ArticlePubMed
 E-submission
E-submission
 , Takeshi Yoshimoto
, Takeshi Yoshimoto

 PubReader
PubReader ePub Link
ePub Link Cite
Cite