 E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 14(3); 2021 > Article
-
Brief communication
Phonatory Characteristics of Male Patients with Classic Essential Tremor -
Preetie Shetty Akkunje1
 , Belur Keshavaprasad Yamini1, Ravi Yadav2, Nagarajarao Shivashankar1, Palash Kumar Malo3, Kandavel Thennarasu3, Shantala Hegde4, Pramod Kumar Pal2
, Belur Keshavaprasad Yamini1, Ravi Yadav2, Nagarajarao Shivashankar1, Palash Kumar Malo3, Kandavel Thennarasu3, Shantala Hegde4, Pramod Kumar Pal2 -
Journal of Movement Disorders 2021;14(3):226-230.
DOI: https://doi.org/10.14802/jmd.21010
Published online: August 18, 2021
1Department of Speech Pathology and Audiology, National Institute of Mental Health and Neurosciences, Bengaluru, India
2Department of Neurology, National Institute of Mental Health and Neurosciences, Bengaluru, India
3Department of Biostatistics, National Institute of Mental Health and Neurosciences, Bengaluru, India
4Department of Clinical Psychology, National Institute of Mental Health and Neurosciences, Bengaluru, India
- Corresponding author: Belur Keshavaprasad Yamini, PhD Department of Speech Pathology and Audiology, National Institute of Mental Health and Neurosciences, Hosur Road, Bengaluru, Karnataka 560029, India / Tel: +91-9980229280 / Fax: +91-80-26995572 / E-mail: yaminihk@gmail.com
Copyright © 2021 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,604 Views
- 94 Download
- 1 Crossref
ABSTRACT
-
Objective
- Voice tremor (VT) is one of the characteristics of essential tremor (ET). This study was designed to describe the group and phonatory characteristics of classic ET patients with VT.
-
Methods
- This retrospective case-control study compared classic ET patients with age and sex-matched controls. The ET population was subgrouped based on auditory perceptual voice analysis. Electroglottography and acoustic voice samples obtained from both groups were analyzed for contact quotient (CQ) and multidimensional voice program parameters, i.e., fundamental frequency (F0), perturbation, noise, and tremor parameters.
-
Results
- The CQ, F0, perturbation, noise, and tremor characteristics significantly increased from the moderate VT group to the severe VT group.
-
Conclusion
- The CQ, F0, and noise characteristics reflected the vocal folds’ functionality. The perturbation and tremor parameters variation were reasoned considering the tremor-related changes occurring in the laryngeal, vocal tract, and expiratory muscles in patients with ET. Thus, phonatory analysis may help in monitoring the progression of ET.
- Participant selection
- The present research is a retrospective case-control study approved by the Institutional Ethics Committee of National Institute of Mental Health and Neurosciences, Bengaluru, India. Recorded speech and voice samples of all individuals diagnosed with neurological disorders, referred for routine voice evaluation, were retrieved from the voice database of the Department of Speech Pathology and Audiology at National Institute of Mental Health and Neurosciences, Bengaluru, India. The data were extracted between 2008 and 2017 and served as a source for the experimental group. All the subjects included had a confirmed diagnosis of ET as per the Consensus statement of the Movement Disorder Society on Tremor and clinical examinations [14]. Inclusion criteria for the experimental group consisted of age between 45–65 years; the first symptom was upper limb tremor or simultaneous onset of the upper limb, head tremor and/or VT; < 10 years duration of ET, no isolated head and VT; ‘off’ medication at the time of voice evaluation; no structural abnormality of vocal folds (VFs) on laryngoscopy; and no history of stroke or any other neurological condition.
- Healthy control (HC) data consisted of recorded voice samples used to establish clinical normative. The data were from both sexes of individuals aged between 18–70 years who were screened and found to have no neurological, otolaryngological, or psychiatric disorders before recording. From this data pool, we selected controls who were matched in age, sex, and language with the experimental group, thus maintaining homogeneity.
- The voice samples were recorded for sustained phonation of vowel /a/ on Computerized Speech Labs 4500 (KAYPENTAX, Lincoln Park, NJ, USA) at a sampling rate of 44,100 Hz using a high-fidelity microphone (SHURE SM-48; Shure Inc., Niles, IL, USA) placed at a 10 cm distance from the mouth [9]. Simultaneous electroglottography (EGG) recordings (model 6103, KAYPENTAX, Lincoln Park, NJ, USA) were obtained with two surface electrodes; an electrode was placed on each of the alae of the thyroid cartilage [2]. Sustained phonation was considered per the standard protocols for the assessment of EVT [4,5,11].
- Subgrouping ET
- Five speech-language pathologists with over ten years of experience rated each sample of phonation on the Vocal Tremor Rating Scale (VTRS) [15] to reclassify the experimental group into subgroups of ET. Voice samples having an interrater agreement of 80% were considered when classifying the severity of VT among samples as follows: 1-no VT (NVT), 2-mild VT, 3-moderate VT, and 4-severe VT.
- Measurement of phonatory characteristics
- The classified phonation samples were trimmed at their onset and offset to obtain a 2-second-long duration of sustained phonation [9]. Parameters were computed using EGG and Multi-Dimensional Voice Program (MDVP) software (ver.5105, KAYPENTAX, Lincoln Park, NJ, USA). The contact quotient (CQ) was measured using EGG. F0, frequency perturbation [jitter (Jitt), smoothened pitch period perturbation quotient (sPPQ), and coefficient of frequency variation (vF0)], amplitude perturbation [shimmer (Shim), smoothened amplitude perturbation quotient (sAPQ), and coefficient of amplitude variation (vAm)], noise [noise to harmonic ratio (NHR) and soft phonation index (SPI)], and tremor parameters [rate of frequency tremor (Fftr), rate of amplitude tremor (Fatr), magnitude of frequency tremor (FTRI), and magnitude of amplitude tremor (ATRI)] were measured with MDVP. Each parameter is described in Supplementary Material 1 (in the online-only Data Supplement).
- Statistical analysis
- Data were analyzed using SPSS v22.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were computed for all the parameters for the HC group and the ET subgroups. The Shapiro-Wilk test was performed to check the normal distribution of data. The Kruskal-Wallis H-test was used to compare the HC group and subgroups of ET patients. Bonferroni (post hoc) corrected p-values (< 0.05) were used for the interpretation during multiple comparisons.
MATERIALS & METHODS
- A total of 308 patients with ET (204 males) were considered for inclusion in the study; of these patients, 69 male patients fulfilled the inclusion criteria. Out of 178 voice samples (102 males) considered as HCs, 69 males (
RESULTS
- In this study, we tried to objectively measure the phonatory characteristics of voice in patients with ET with varying VT severity. The mean ages of NVT patients and severe VT patients were 51.3 and 60.4 years, respectively. Similar findings on EVT suggest that older individuals exhibit moderate to severe VT [4-6,11]. We considered the duration between the age of ET onset and EVT onset as the transition period (Table 1). The transition period was shorter for the moderate and severe VT groups than for the mild VT group.
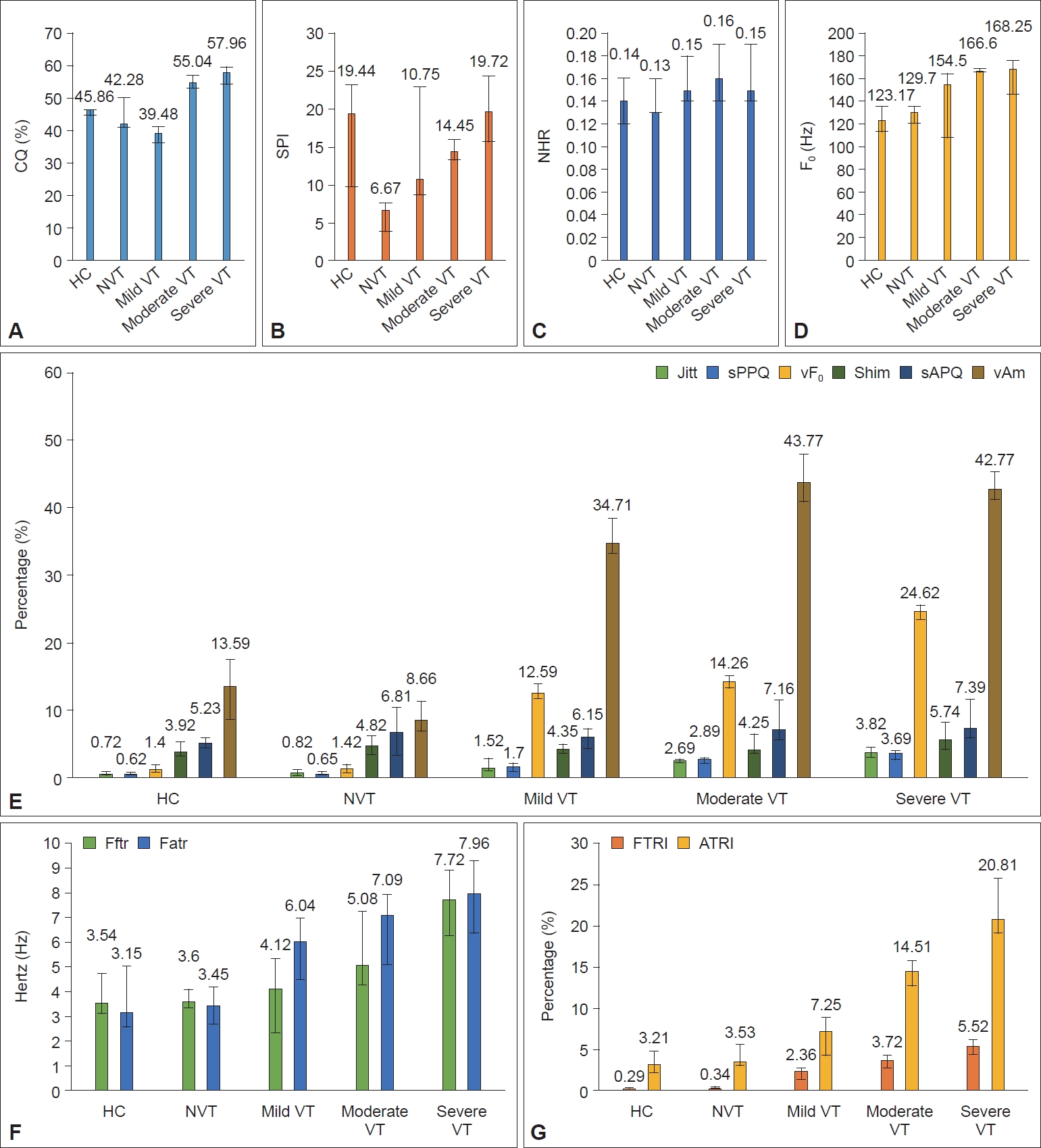
- Sustained phonation results from medialization of the VF by the cricothyroid (adductor) and thyroarytenoid with constant subglottal pressure [16]. The CQ reflects VF medialization (adduction), the SPI determines the completeness of VF closure, and NHR indicates noise (air escape) in the voice signal due to incomplete VF closure [2,16-18]. The CQ was reduced in NVT patients and mild VT patients and increased with the severity of VT. However, the SPI and NHR showed a reduction in NVT patients (< HCs) and reached HC values with tremor severity. We hypothesize that reduced values of the CQ, SPI, and NHR in NVT patients may indicate hypoadduction of the VF, as reported in cases with hypokinetic dysarthria [2,16,17]. Although the CQ was lower in patients with mild VT (compared to patients with NVT), SPI and NHR values were higher, which may indicate reduced contact time between VFs with complete closure (SPI) and negligible air escape (NHR). However, an increase in tremor severity caused VFs to hyperadduct (>CQ) but these patients had complete VF closure (normal SPI) and the least noise (NHR). Adduction of VFs and maintenance of subglottal pressure occurs due to activation of the prefrontal cortex, periaqueductal gray, nucleus retroambiguus, and motor neural pathway [19], which are components of the CON [7]. Thus, the faulty neural impulse to the thyroarytenoid causes postural tremor, which may disrupt constant subglottal pressure to maintain sustained phonation.
- A pitch (F0) change is achieved by altering the length, mass, and tension of VFs caused by cricothyroid and thyroarytenoid muscles (CT-TA) [16]. Frequency perturbation reflects VF vibration and respiratory aerodynamics, whereas amplitude perturbation reflects glottal closure during phonation [18]. Electromyography and pulmonary functions in EVT patients have shown deficits in CT-TA and expiratory (rectus abdominis and pectoralis) muscles of phonation [2,20], respectively.
- In our study, the increase in F0 with the severity of VT suggests elongation of VFs, as substantiated by videostroboscopy studies [4], in addition to a decrease in mass and increase in tension of CT-TA [4]. We also obtained higher values of frequency perturbation (Jitt, sPPQ, and vF0) and amplitude perturbation (Shim, sAPQ, and vAm) in patients with moderate and severe VT, similar to findings in the literature [5]. We hypothesize that changes in muscle tone and stiffness of CT-TA in addition to an imbalance between subglottal and supraglottal pressure are the reason for abnormal frequency and amplitude perturbation values.
- Modulation seen in phonation occurs due to activation of corticobulbar fibers that project to mouth, face, laryngeal, and pharyngeal motoneurons [19]. The tremor parameters (Fftr, Fatr, FTRI, and ATRI) [9] determine the strongest periodic modulation of frequency and amplitude in voice. Our study showed an increase in tremor parameters with the severity of VT. We hypothesize that the abnormal tremor parameters could be from oscillations in intrinsic and extrinsic laryngeal muscles, the vocal tract, and respiratory muscles (diaphragm, rectus abdominis, and pectoralis) [2]; these oscillations may induce modulation in glottal airflow.
- Our findings can help clinicians quantify patients’ voice characteristics with ET rather than them having to rely on perceptual evaluation alone. This may help clinicians monitor the progression of the disorder by analyzing the deterioration of voice quality and may also serve as a baseline for intervention studies.
DISCUSSION
Supplementary Materials
SUPPLEMENTARY MATERIAL 1
Supplementary Table 1.
-
Conflicts of Interest
The authors have no financial conflicts of interest.
-
Funding Statement
None.
-
Author Contributions
Conceptualization: Preetie Shetty Akkunje, Belur Keshavaprasad Yamini, Nagarajarao Shivashankar. Data curation: Preetie Shetty Akkunje, Belur Keshavaprasad Yamini, Ravi Yadav, Nagarajarao Shivashankar, Palash Kumar Malo, Kandavel Thennarasu. Formal analysis: Preetie Shetty Akkunje, Belur Keshavaprasad Yamini, Ravi Yadav, Nagarajarao Shivashankar, Shantala Hegde, Pramod Kumar Pal. Investigation: Preetie Shetty Akkunje, Belur Keshavaprasad Yamini, Ravi Yadav, Nagarajarao Shivashankar, Shantala Hegde, Pramod Kumar Pal. Methodology: all authors. Project administration: Belur Keshavaprasad Yamini, Ravi Yadav, Nagarajarao Shivashankar, Pramod Kumar Pal. Resources: Belur Keshavaprasad Yamini, Ravi Yadav, Nagarajarao Shivashankar, Kandavel Thennarasu, Pramod Kumar Pal. Software: Belur Keshavaprasad Yamini, Ravi Yadav, Nagarajarao Shivashankar, Kandavel Thennarasu, Pramod Kumar Pal. Supervision: Belur Keshavaprasad Yamini, Ravi Yadav, Nagarajarao Shivashankar, Kandavel Thennarasu, Shantala Hegde, Pramod Kumar Pal. Validation: all authors. Visualization: Belur Keshavaprasad Yamini, Ravi Yadav, Nagarajarao Shivashankar, Kandavel Thennarasu, Shantala Hegde, Pramod Kumar Pal. Writing—original draft: Preetie Shetty Akkunje. Writing—review & editing: all authors.
Notes
- Authors thank Mr. Prashasti P. Poovaiah for his assistance.
Acknowledgments
| Group characteristics | ET as a group (n = 69) |
Subgroups of ET |
||||
|---|---|---|---|---|---|---|
| NVT (n = 14) | Mild VT (n = 15) | Moderate VT (n = 12) | Severe VT (n = 28) | p-value | ||
| Mean age (years) | 56.9 ± 6.7 | 51.3 ± 6.9 | 55.3 ± 6.7 | 57.6 ± 7.1 | 60.4 ± 4.1 | 0.001* |
| Duration of essential tremor (years) | 3.5 ± 1.9 | 4.7 ± 1.8 | 2.8 ± 1.7 | 3.8 ± 1.6 | 3.1 ± 1.1 | 0.019* |
| Age of essential tremor onset (years) | 53.6 ± 7.1 | 46.7 ± 7.9 | 52.5 ± 7.3 | 53.8 ± 7.2 | 57.3 ± 4.9 | 0.001* |
| Duration of essential voice tremor (years) | 2.3 ± 1.6 | - | 1.7 ± 0.7 | 2.6 ± 1.6 | 2.3 ± 1.7 | - |
| Age of essential voice tremor onset (years) | 57.6 ± 5.3 | - | 59 ± 3.7 | 55.9 ± 6.9 | 58.1 ± 4.8 | - |
| Family history | 40.5 (28) | 50 (7) | 60 (9) | 41.6 (5) | 25 (7) | - |
| Bilateral upper limb tremor (AE) | 100 (69) | 100 (14) | 100 (15) | 100 (12) | 100 (28) | - |
| Bilateral lower limb tremor (AE) | 73.9 (51) | 28.6 (4) | 46.7 (7) | 100 (12) | 100 (28) | - |
| Head tremor (AE) | 37.9 (26) | - | 14.3 (2) | 41.7 (5) | 67.9 (19) | - |
| Tongue tremor (AE) | 26.1 (18) | 7.1 (1) | 20 (3) | 33.3 (4) | 35 (10) | - |
- 1. Louis ED, Gerbin M, Galecki M. Essential tremor 10, 20, 30, 40: clinical snapshots of the disease by decade of duration. Eur J Neurol 2013;20:949–954.ArticlePubMedPMC
- 2. Sataloff RT. Neurolaryngology. San Diego: Plural Publishing; 2017:181–737.181-208, 299-332, 655-681, 715-737.
- 3. Sulica L, Louis ED. Clinical characteristics of essential voice tremor: a study of 34 cases. Laryngoscope 2010;120:516–528.ArticlePubMed
- 4. Lester RA, Barkmeier-Kraemer J, Story BH. Physiologic and acoustic patterns of essential vocal tremor. J Voice 2013;27:422–432.ArticlePubMed
- 5. Gamboa J, Jiménez-Jiménez FJ, Nieto A, Cobeta I, Vegas A, Ortí-Pareja M, et al. Acoustic voice analysis in patients with essential tremor. J Voice 1998;12:444–452.ArticlePubMed
- 6. Paige C, Hopewell BL, Gamsarian V, Myers B, Patel P, Garrett CG, et al. Characterizing the normative voice tremor frequency in essential vocal tremor. JAMA Otolaryngol Head Neck Surg 2018;144:1169–1173.ArticlePubMedPMC
- 7. Raethjen J, Deuschl G. The oscillating central network of essential tremor. Clin Neurophysiol 2012;123:61–64.ArticlePubMed
- 8. Simonyan K, Horwitz B. Laryngeal motor cortex and control of speech in humans. Neuroscientist 2011;17:197–208.ArticlePubMedPMC
- 9. Kent RD, Vorperian HK, Kent JF, Duffy JR. Voice dysfunction in dysarthria: application of the multi-dimensional voice program. J Commun Disord 2003;36:281–306.ArticlePubMed
- 10. Lederle A, Barkmeier-Kraemer J, Finnegan E. Perception of vocal tremor during sustained phonation compared with sentence context. J Voice 2012;26:668.e1–e9.ArticlePubMed
- 11. Suppa A, Asci F, Saggio G, Di Leo P, Zarezadeh Z, Ferrazzano G, et al. Voice analysis with machine learning: one step closer to an objective diagnosis of essential tremor. Mov Disord 2021;36:1401–1410.ArticlePubMed
- 12. Rao Mv A, Yamini BK, Ketan J, Preetie Shetty A, Pal PK, Shivashankar N, et al. Automatic classification of healthy subjects and patients with essential vocal tremor using probabilistic source-filter model based noise robust pitch estimation. J Voice 2021;Feb. 9. [Epub]. Available from: https://doi.org/10.1016/j.jvoice.2021.01.009. Article
- 13. Barkmeier-Kraemer JM. Isolated voice tremor: a clinical variant of essential tremor or a distinct clinical phenotype? Tremor Other Hyperkinet Mov (N Y) 2020;Jan. 23. [Epub]. Available from: https://doi.org/10.7916/tohm.v0.738. Article
- 14. Deuschl G, Bain P, Brin M; Ad Hoc Scientific Committee. Consensus statement of the movement disorder society on tremor. Mov Disord 2008;13 Suppl 3:2–23.Article
- 15. Bassich CJ, Ludlow CL. The use of perceptual methods by new clinicians for assessing voice quality. J Speech Hear Disord 1986;51:125–133.ArticlePubMed
- 16. Raphael LJ, Borden GJ, Harris KS. Speech Science Primer: Physiology, Acoustics, and Perception of Speech. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2007:42–113.
- 17. Mathieson L. Greene and Mathieson’s the Voice and its Disorders. 6th ed. New York: John Wiley & Sons; 2013:268–324.
- 18. Baken RJ. Clinical Measurement of Speech and Voice. 2nd ed. Austin: Pro-Ed; 1987:145–223.
- 19. Holstege G, Subramanian HH. Two different motor systems are needed to generate human speech. J Comp Neurol 2016;524:1558–1577.ArticlePubMed
- 20. Jiménez-Jiménez FJ, Izquierdo-Alonso JL, Cabrera-Valdivia F, Mansilla-Lesmes M, Martínez-Martín P, Serrano-Iglesias JA. Dysfunction of the upper respiratory airways in patients with essential tremor. Presse Med 1995;24:1152–1156.PubMed
REFERENCES
Figure & Data
References
Citations
- Voice Analysis in Patients with Essential Tremor
Hakan Silek, Muzeyyen Dogan
Journal of Voice.2023;[Epub] CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite
