Letter to the editor Genetically Proven Ataxia With Vitamin E Deficiency With Predominant Cervicobrachial Dystonic Presentation: A Case Report From India
1Department of Neurology, National Institute of Mental Health and Neurosciences, Bengaluru, India
2Department of Human Genetics, National Institute of Mental Health and Neurosciences, Bengaluru, India
Corresponding author: Pramod Kumar Pal, MD, DNB, DM, FRCP Department of Neurology, National Institute of Mental Health and Neurosciences, Hosur Road, Bengaluru, Karnataka 560029, India / Tel: +91-80-26995147 / Fax: +91-80-26564830 / E-mail: palpramod@hotmail.com
• Received: November 5, 2023 • Revised: November 28, 2023 • Accepted: December 16, 2023
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Ataxia with vitamin E deficiency (AVED) is a rare potentially treatable autosomal recessive disorder [1-3]. AVED is caused by a biallelic mutation in the TTPA gene, which encodes the alphatocopherol transfer protein (αTTP). αTTP is involved in transporting vitamin E out of the liver into tissues through its incorporation into very-low-density lipoprotein. In AVED, the intestinal absorption of vitamin E is intact, but the circulating level in blood is very low. It typically presents from childhood to adolescence with a Friedreich ataxia (FA)-like phenotype characterized by ataxia, areflexia, and loss of proprioceptive and vibratory sensations. Head titubation is frequently associated with this disease, but dystonic head tremor as the predominant symptom is infrequently reported [1,3-5]. We report a biochemically and genetically proven case of early adult-onset AVED presenting with predominant cervical and upper-limb dystonic tremor and sensory predominant ataxia.
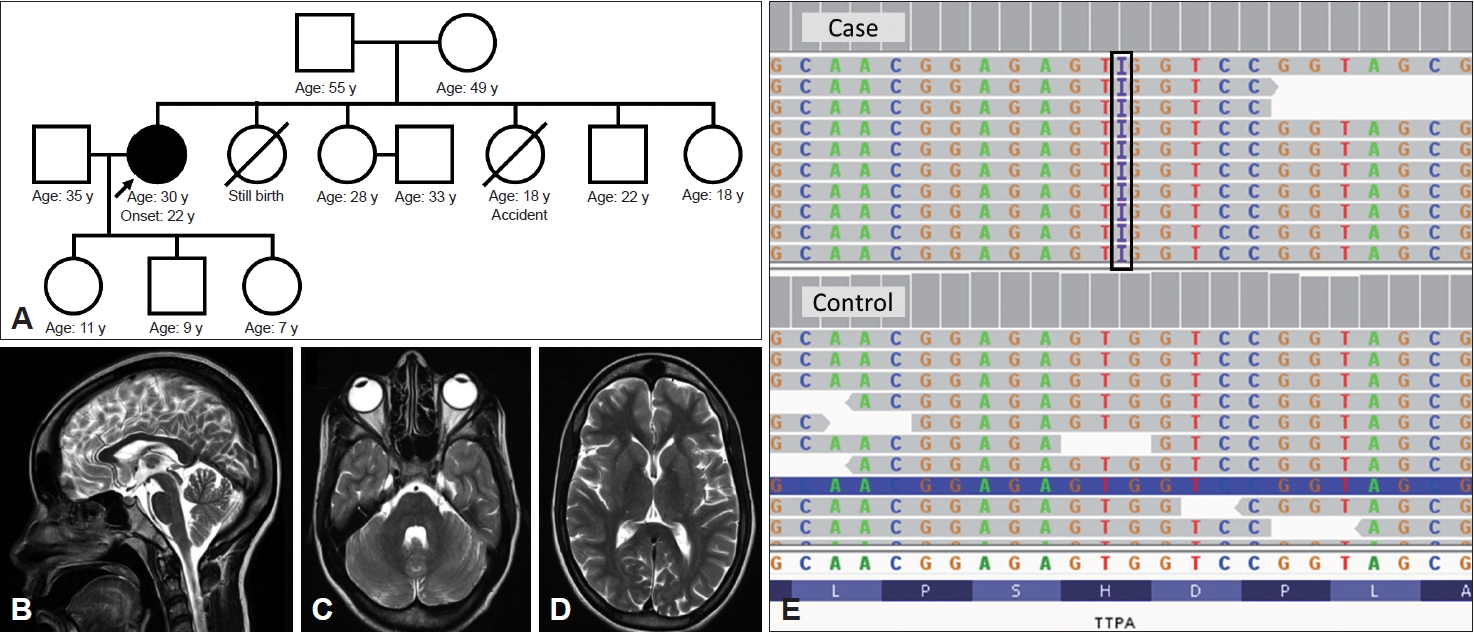
A 30-year-old female patient born to nonconsanguineous parents with an otherwise normal perinatal, developmental, and family history (Figure 1A) presented with tremulousness of the head and left upper limb for eight years and walking difficulty for six years. Tremulousness of the head was decreased when lying down; both yes-yes and no-no types of tremors were observed at different times; tremors were reduced when looking to the right; and abnormal posturing of the neck was reduced with a sensory trick (Supplementary Video 1 in the online-only Data Supplement). The patient had upper-limb tremors at rest and during activity, the latter of which were historically more severe and worsened when reaching for objects. Additionally, she also reported abnormal posturing of the right hand at rest and during activity. While walking, she swayed to either side, and the swaying was more common at night and when she closed her eyes. She denied any symptoms in the right upper limb, and there were no other relevant neurological or systemic symptoms. Informed consent was obtained for video recording and publication.
The patient had normal cognition and cranial nerve examination results, including visual acuity, fundus and eye movements. The head tremors were predominantly of the no-no type with mild lateral tilt and lateral shift of the head when sitting comfortably with a null point (Supplementary Video 1 in the online-only Data Supplement). In addition, dystonia of the left hand along with pronation supination tremor of the left forearm could be observed both at rest and during posture and activity. Incoordination was observed in the left-side predominant finger nose test, and there was no significant dysdiadokokinesia. The heel-shin test indicated bilateral impairment, which was better with visual cues. Head tremor was more apparent when walking, and truncal dystonia and mild right foot dystonia were observed. Additionally, the patient exhibited generalized hyporeflexia, reduced vibration sensation at the bilateral medial malleolus, impaired proprioception at the bilateral great toe, impaired tandem gait and a positive Rhomberg sign with otherwise normal tone, power and bilateral flexor plantar response. The rest of the examination results were normal.
Routine blood investigation results; vitamin B12, folate, homocysteine, ammonia, and lactate levels; and abnormal metabolites screening results were normal. A sensory-motor nerve conduction study (NCS) of all four limbs yielded normal results, whereas visual, brainstem auditory and somatosensory-evoked potential studies revealed prolonged latency in the lower limbs alone. Magnetic resonance imaging (MRI) of the brain and spine screening was normal (Figure 1B-D). Head titubation, sensory predominant ataxia and a normal cerebellum on MRI suggested the possibility of an FA phenotype. GAA repeat test for FA were negative, but the blood level of vitamin E was extremely low (178.081 ng/mL; normal: 5,500–18,000 ng/mL). Whole-exome sequencing confirmed the diagnosis of AVED; a homozygous variant previously reported in ClinVar (SCV003204819.1), a pathogenic 1-bp duplication in the TTPA gene (chr8:g.63085963insG [GRCh38]; NM_000370.3:c.58dupC; p.His20ProfsTer56), was detected (Figure 1E). The patient was treated with 1,200 IU/day of vitamin E along with symptomatic therapy for dystonia with clonazepam and trihexyphenidyl. At the 3-month follow-up, there was no further worsening or clinical improvement.
AVED usually manifests around late childhood to early adolescence, but patients with onset from early childhood to the fourth decade have been reported [1]. AVED presents clinically with an FA-like phenotype, and > 90% of patients have progressive ataxia, hyporeflexia and/or impaired proprioception at the time of presentation; additionally, pyramidal signs and skeletal abnormalities can occur. In contrast to FA, head tremor is a frequent occurrence in AVED, occurring in approximately one-third to two-thirds of patients at presentation [4], and patients with AVED have less severe neuropathy, less frequent cardiac involvement, and lower occurrence of kyphoscoliosis and diabetes than patients with FA. Rarely, dystonia and myoclonus have also been reported in AVED [6]. In most patients, head tremor is secondary to head titubation due to cerebellar involvement. Becker et al. [3] reported 2 patients with dystonic head tremor as the presenting symptom in a family with AVED. In addition, they reviewed the literature and identified 10 additional cases of AVED in which dystonia was noted. Pradeep et al. [5] reported two out of three siblings from a family with AVED who had predominant dystonic head tremor at onset followed by the development of other features of AVED. Subsequently, there are two additional reports [7,8] of dystonia in patients with AVED (Supplementary Table 1 in the online-only Data Supplement). Among the cases reported to date, including ours, the common trend is that dystonia predominantly involves the neck in more than three-fourths of patients, followed by the upper limbs and lower limbs; dystonia eventually generalizes in approximately 50% of patients, and although it can be the first symptom, it is never isolated, as it is always associated with other features of AVED, such as ataxia, hyporeflexia and/or proprioceptive impairment.
Neuronal oxidative injury due to vitamin E deficiency has been postulated to be the mechanism of neurological dysfunction in AVED [1,3]. Animal models of AVED and tissue histopathology and postmortem studies in humans have demonstrated degenerative changes in the substantia nigra, loss of Purkinje cells in the cerebellum, and dying back-type posterior column degeneration, with or without involvement of nerve roots or the peripheral nervous system [3]. Ataxia in AVED is likely to occur through a combination of cerebellar and posterior column involvement. Mild nonspecific cerebellar atrophy can be observed on brain MRI in up to 50% of patients. Electrophysiological studies demonstrate prolonged sensory conduction time for somatosensory-evoked potentials; NCS often reveals sensory and/or motor axonal injury but can be normal in approximately 10% of cases [1,6]. Early diagnosis is important so that high-dose vitamin E supplementation can be initiated early to halt disease progression and, in some cases, cause clinical improvement, especially in patients with shorter disease duration. Without treatment, patients with AVED can become wheelchair bound due to ataxia and/or leg weakness within 5–20 years, especially if the onset was early [1,3]. Ataxia and intellectual deterioration can be reversed in symptomatic individuals if supplementation is started early in the disease course, whereas in older individuals, cessation of disease progression can be expected, although proprioception and gait abnormalities may persist [1]. The response of dystonia to vitamin E supplementation is variable, with improvement in most patients, stabilization in a few patients and progressive dystonia despite supplementation in 1 patient [3]. At the 3-month follow-up, the symptoms had stabilized in our patient. However, a longer follow-up is necessary to fully understand the effect of vitamin E supplementation.
In conclusion, cervicobrachial dystonia with dystonic tremor can be a predominant feature in patients with AVED. This knowledge will aid in early diagnosis and prompt initiation of vitamin E supplementation.
Video of the patient. The patient demonstrated normal eye movements; no-no head tremor with mild left tilt and head shift, worsening of head tremor when looking to the left or looking down, improvement when looking to the right and almost no tremor when looking up; dystonia of the left hand along with pronation supination tremor of the left forearm both at rest and in posture and activity; impairment in the left-side predominant bilateral finger nose test; no significant dysdiadokokinesia; impairment in the heel-shin test; more apparent head tremor along with truncal dystonia and mild right foot dystonia on walking; and impaired tandem gait.
Supplementary Table 1.
Clinical characteristics and treatment response in patients with AVED and dystonia
The authors confirm that the Institutional Review Board of NIMHANS Ethics Committee waiver was obtained for this work (No. NIMHANS/IEC/2023). We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines. The video of the patient was taken after written informed consent for video recording and for publication both in print and online.
Conflicts of Interest
The authors have no financial conflicts of interest.
Funding Statement
None
Author contributions
Conceptualization: Vikram V. Holla, Pramod Kumar Pal. Data curation: Vikram V. Holla, Sandeep Gurram, Sneha D. Kamath, Gautham Arunachal. Formal analysis: Vikram V. Holla, Pramod Kumar Pal. Investigation: Vikram V. Holla, Nitish Kamble, Pramod Kumar Pal. Supervision: Nitish Kamble, Ravi Yadav, Pramod Kumar Pal. Writing—original draft: Vikram V. Holla. Writing—review & editing: Sandeep Gurram, Sneha D. Kamath, Gautham Arunachal, Nitish Kamble, Ravi Yadav, Pramod Kumar Pal.
Figure 1.
Pedigree, MRI brain and snapshot of the variant identified in the patient. A: Pedigree of the proband. B-D: T2 sequences of the brain MRI of the patient demonstrating normal cerebellum, corpus callosum, and basal ganglia structures. E: Integrated Genome Viewer snapshot of the BAM file at the region of interest in the patient and a control demonstrating homozygous insertion (I, black box) of a nucleotide (G) at locus chr8:g.63085963 (GRCh38 reference genome) that results in the c.58dupC variant. MRI, magnetic resonance imaging.
REFERENCES
1. Schuelke M. Ataxia with vitamin E eeficiency [Updated 2023 Mar 16]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, et al. GeneReviews® [Internet]. Seattle: University of Washington. c1993-2024. [accessed on 2023 Nov 4]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1241/.
2. Stezin A, Pal PK. Treatable ataxias: how to find the needle in the haystack? J Mov Disord 2022;15:206–226.ArticlePubMedPMCPDF
3. Becker AE, Vargas W, Pearson TS. Ataxia with vitamin E deficiency may present with cervical dystonia. Tremor Other Hyperkinet Mov (N Y) 2016;6:374.ArticlePubMedPMC
4. El Euch-Fayache G, Bouhlal Y, Amouri R, Feki M, Hentati F. Molecular, clinical and peripheral neuropathy study of Tunisian patients with ataxia with vitamin E deficiency. Brain 2014;137(Pt 2):402–410.ArticlePubMed
5. Pradeep S, Ali T, Guduru Z. Ataxia with vitamin E deficiency with predominant cervical dystonia. Mov Disord Clin Pract 2019;7:100–103.ArticlePubMedPMCPDF
6. Mariotti C, Gellera C, Rimoldi M, Mineri R, Uziel G, Zorzi G, et al. Ataxia with isolated vitamin E deficiency: neurological phenotype, clinical follow-up and novel mutations in TTPA gene in Italian families. Neurol Sci 2004;25:130–137.ArticlePubMedPDF
7. Zea Vera A, Liu W, Thomas C, Gilbert DL. Pearls & oy-sters: a novel presentation of ataxia with vitamin E deficiency caused by TTPA gene mutation. Neurology 2021;96:e640–e642.ArticlePubMed
8. Zhang LW, Liu B, Peng DT. Clinical and genetic study of ataxia with vitamin E deficiency: a case report. World J Clin Cases 2022;10:8271–8276.ArticlePubMedPMC
 E-submission
E-submission
 , Sandeep Gurram1
, Sandeep Gurram1

 PubReader
PubReader ePub Link
ePub Link Cite
Cite
