This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Task-specific oromandibular tremor is present only while the patient is performing a special task. Many cases are medically intractable, and the therapy of choice has been botulinum toxin (BoNT) injections.
We report the case of a 63-year-old female with a sudden onset of task-specific oromandibular tremor who could suddenly not drink from a cup or glass without spillage of the fluid. The condition was refractory for over a year. After interdisciplinary clinical and electrophysiological examinations, the patient received BoNT-A injections in the superior and inferior orbicularis oris muscles and later to the digastricus muscles, and her tremor diminished markedly. Thus, the patient rated the negative impact from the condition after treatment as a 5 on a nominal rating scale (NRS 0 to 10), whereas she had rated it as a 9 before the injections. Our findings stress the importance of multidisciplinary clinical and electromyographic examinations of severe and intractable oromandibular tremors.
Task-specific lip tremor is a rare form of oromandibular dystonia characterized by involuntary, rhythmic oscillation of the perioral muscles triggered by performing a specific task. This condition is incapacitating and socially stigmatizing in nature. The etiology is often idiopathic. The efficacy of BoNT A injections in task-specific tremor is sparse [1], but there are studies reporting improvement in up to 80% of cases and a superior effect compared to primidone or propranolol. Our patient was refractory to medicine and showed no improvement after previous BoNT injections for a year.
We report a 63-year-old, left-handed Caucasian female with sudden-onset, progressive oromandibular tremor and drinking difficulty. The symptoms started in relation to an unexpected change in her working situation. She felt stressed and had little time to eat and drink. One day feeling thirsty, she lifted a water bottle, but when it touched her mouth, she could not drink because of tremor. Instead, she spilled a large amount of water. The tremor immediately disappeared when she stopped her drinking efforts. Ever since, she has experienced severe drinking difficulty and more intensely when stressed. First, the tremor was provoked only by drinking from a bottle and later became present when attempting to drink from a glass, but she could drink with a straw without problems. At the time of her symptom debut, she was taking clomipramine 25 mg/day for anxiety and certizine 10 mg/day for allergies.
Prior to referral to the Bispebjerg University Hospital, treatment with oral clonazepam 10 mg/day and propranolol 30 mg/day did not alleviate the tremor. Intramuscular BoNT-A was also administered previously to the temporalis, masseter and lateral pterygoid muscles with doses up to 30 units/muscle without effect.
At admittance, the examination revealed tremor of the jaw and the perioral muscles but only if a glass or bottle was in contact with her mouth (Supplementary Video 1 in the online-only Data Supplement). The tremor also sometimes involved the left arm and hand. The patient was able to whistle and eat without tremor, and there was normal mobility of the jaw without pain. She did not experience tremor of either the hand or the mouth in other situations. No stiffness or slowness of the limbs or walking difficulties were found, nor were sleeping disturbances, headache or temporomandibular disorders. Magnetic resonance imaging of the brain was also normal.
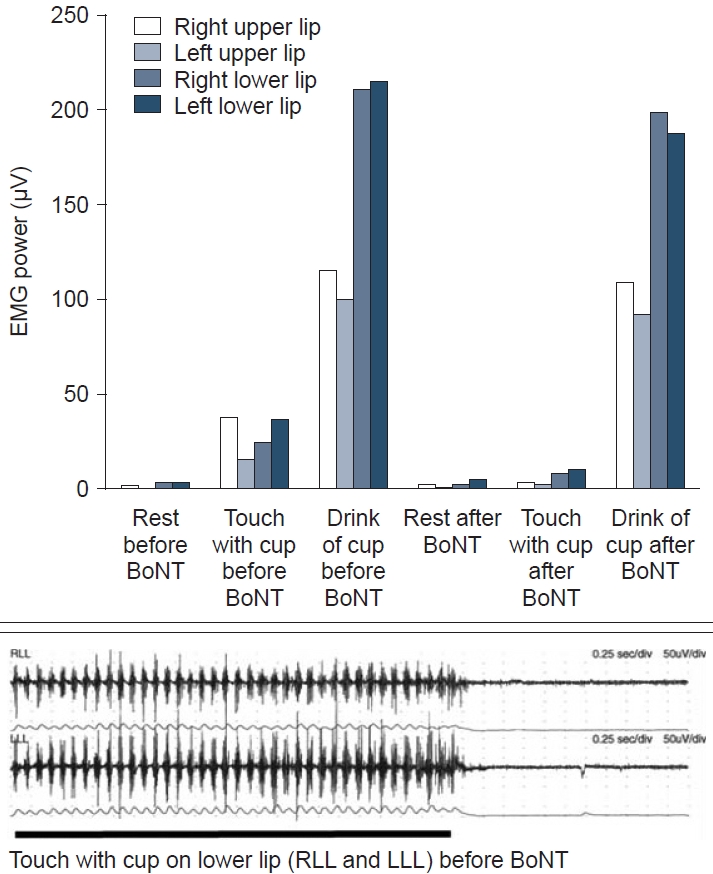
Because of the previous poor response to treatment, we performed detailed electromyographic analyses (EMG). Recordings of the masseter, temporal and anterior belly of the digastricus muscles showed no burst activity in either the relaxed position or during talking or drinking (Figure 1). Drinking from a cup or touching of the lips with a cup or glass started irregular 4–7 Hz tremor bursts and increased the average activity level from the orbicularis oris muscles [2]. Therefore, BoNT-A (incobotulinum toxin A) was injected into each side of the orbicularis oris superior (8–8 IU) and inferior (10–10 IU). Two weeks after treatment, we observed an amplitude reduction of the tremor bursts on control EMG and average amplitudes in both the superior and inferior parts of the orbicularis oris (Figure 1). At an evaluation 3 months after the injections, the patient rated her tremor on a NRS for negative impact (0 to 10) as a 7 for approximately one month, which had changed from an initial value of 9 [3]. After supplementing the treatment with injections of the anterior part of the digastricus muscles (12–12 IU), the improvement was rated by the patient as a 5, which slowly progressed again for a 2-month period until it reached an NRS value of 9 again.
After obtaining this information, the patient gave written consent for publication.
Our case was an idiopathic lip tremor that was relieved after interdisciplinary detailed clinical and electrophysiological examinations. Such tremor has been previously associated with Parkinson’s disease [4]; however, our patient did not show any other sign of extrapyramidal symptoms, and there was no disposition for extrapyramidal disorders in her family. Essential tremor is also unlikely because of the sudden onset and the exclusive appearance of the tremor during drinking. The etiology in our case remains idiopathic. Our patient is intriguing because, despite several previous clinical investigations and the use of different types of medication, she was medically intractable and experienced almost no improvement.
The use of EMG-guided BoNT-A treatment of dystonia has been broadly discussed. However, electrophysiological investigation is playing an increasing role in tremor characterization because many aspects of tremor cannot be assessed clinically [5]. Difficulty with drinking may be a sign of tremor, and EMG assessment can be used to visualize and compare the activity of the muscles closely related to functions, such as drinking. Our case also demonstrates that significant clinical alleviation can be obtained with EMG and tremor burst analysis. Our findings are in accordance with other reports that found EMG recordings to be useful in evaluating oromandibular dystonia (e.g. [6], ), in assessing tremor and in monitoring the treatment effect [7].
Jaw tremor can be a symptom in various disorders. Therefore, we suggest that the EMG findings are always assessed side-by-side with thorough interdisciplinary clinical evaluation and with the patient’s subjective judgment of life quality before and after treatment.
Supplementary Video Legends
Video 1.
Video showing the patient’s face when at rest, licking the lips, counting to ten, eating a slice of apple, and drinking water with a straw, which are all situations without dystonia, and when drinking water from a glass provoking dystonic tremor.
We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines. Our patient was informed and signed an informed consent form for publishing her data and video file.
Conflicts of Interest
The authors have no financial conflicts of interest.
The diagram at the top shows the activity level of lip muscles (mean rectified amplitude recorded with bipolar surface electrodes). 7 The columns represent the average of the mean activity in 3 epochs of 10 s at rest and with a cup touching the lips and the average of the peak amplitude during drinking in 2 epochs. There was a general 78% reduction during touch and 8% reduction during drinking after treatment, whereas the activity was almost unchanged during rest. Below, the raw electromyographic recordings from the RLL and LLL and their mean rectified amplitude show the burst activity in response to the touch of the cup and the resting activity afterward.7 The EMG data show the variability of the peak frequency and instability of tremor bursts over time, suggesting a dystonic tremor. EMG, electromyographic analyses; BoNT, botulinum toxin; RLL, right lower lip; LLL, left lower lip.
REFERENCES
1. Mittal SO, Lenka A, Jankovic J. Botulinum toxin for the treatment of tremor. Parkinsonism Relat Disord 2019;63:31–41.ArticlePubMed
2. Møller E, Werdelin LM, Bakke M, Dalager T, Prytz S, Regeur L. Treatment of perioral dystonia with botulinum toxin in 4 cases of Meige’s syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:544–549.ArticlePubMed
3. Bakke M, Henriksen T, Biernat HB, Dalager T, Møller E. Interdisciplinary recognizing and managing of drug-induced tardive oromandibular dystonia: two case reports. Clin Case Rep 2018;6:2150–2155.ArticlePubMedPMCPDF
4. Erer S, Jankovic J. Hereditary chin tremor in Parkinson’s disease. Clin Neurol Neurosurg 2007;109:784–785.ArticlePubMed
5. Tucker H, Osei-Poku F, Ashton D, Lally R, Jesuthasan A, Latorre A, et al. Management of secondary poor response to botulinum toxin in cervical dystonia: a multicenter audit. Mov Disord Clin Pract 2021;8:541–545.ArticlePubMedPMCPDF
6. Everlo CSJ, Elting JWJ, Tijssen MAJ, Madelein van der Stouwe AM. Electrophysiological testing aids the diagnosis of tremor and myoclonus in clinically challenging patients. Clin Neurophysiol Pract 2022;7:51–58.ArticlePubMedPMC
7. Bakke M, Larsen BM, Dalager T, Møller E. Oromandibular dystonia--functional and clinical characteristics: a report on 21 cases. Oral Surg Oral Med Oral Pathol Oral Radiol 2013;115:e21–e26.Article
Figure & Data
References
Citations
Citations to this article as recorded by
A mini-review of the pathophysiology of task-specific tremor: insights from electrophysiological and neuroimaging findings Yih-Chih Jacinta Kuo, Kai-Hsiang Stanley Chen Dystonia.2023;[Epub] CrossRef
 E-submission
E-submission

 , Heidi Bryde Biernat2, Carsten Eckhart Thomsen3, Merete Bakke3
, Heidi Bryde Biernat2, Carsten Eckhart Thomsen3, Merete Bakke3 

 PubReader
PubReader ePub Link
ePub Link Cite
Cite