Recurrent ADCY5 Mutation in Mosaic Form with Nocturnal Paroxysmal Dyskinesias and Video Electroencephalography Documentation of Dramatic Response to Caffeine Treatment
Article information

Dear Editor,
Primary paroxysmal dyskinesias (PxDs) are a highly heterogeneous group of disorders with several causative genes. Mutations in one such gene, ADCY5, commonly present with dystonia, chorea, myoclonus or a combination of the above [1-3]. Neurological manifestations of ADCY5 mutations include the following core clinical features: continuous dyskinesias, ballistic bouts, paroxysmal sleep-related dyskinesias and axial hypotonia. Other rare symptoms include cognitive impairment, psychiatric symptoms, etc. Rarely, nonneurological manifestations including cardiomyopathy have been reported. Various drug treatments have been attempted with only modest responses; however, a dramatic response to caffeine was recently reported [4,5]. We would like to report a patient with a mosaic mutation in ADCY5 presenting with pure PxD and a dramatic response to caffeine therapy.
A 32 year-old male born to nonconsanguineous parentage with no history of perinatal birth injury presented in November 2018 with paroxysmal involuntary movements during sleep from the age of 4 years. For each paroxysmal event, arousal from sleep occurred just before the motor phenomenon, as noted by onset of posterior alpha rhythm on video electroencephalography (video EEG). This was followed by involuntary movements consisting of generalized non-patterned choreiform with dystonic movements, better described as generalized dyskinesia or ‘ballistic bouts.’ [4] Each event lasted approximately 3 minutes with preserved awareness throughout the event confirmed by clinical assessment (Supplementary Video 1 and 2 in the online-only Data Supplement). The patient experienced similar events during daytime naps. The patient experienced approximately 20–30 events per night (cumulating to 60–90 minutes of involuntary movements per night). The events more often occurred in early morning hours and in winter. Interictal examination, MRI brain scan and basic metabolic work-up were normal. In view of a classical history of long-standing, exclusively sleep-related, brief paroxysmal dyskinesia without any movement/exercise related triggers, PxD related to a de novo ADCY5 mutation (in view of a negative family history) was clinically diagnosed over other clinical differentials. Whole exome sequencing was performed due to the genetic heterogeneity of PxD. A known pathogenic variant was identified in the ADCY5 gene (NM_183357.2:Exon 2:c.1252C > T:p.R418W). Further exome data analysis revealed that the variant was mosaic with low mutant read depth (Total depth: 85, Wildtype: 72, Mutant: 13). The effect of this variant was tested according to the American College of Medical Genetics and Genomics (ACMG) standards and guidelines. The variant was confirmed by Sanger sequencing in the proband. The parents were found to be homozygous for the wildtype allele (Figure 1).
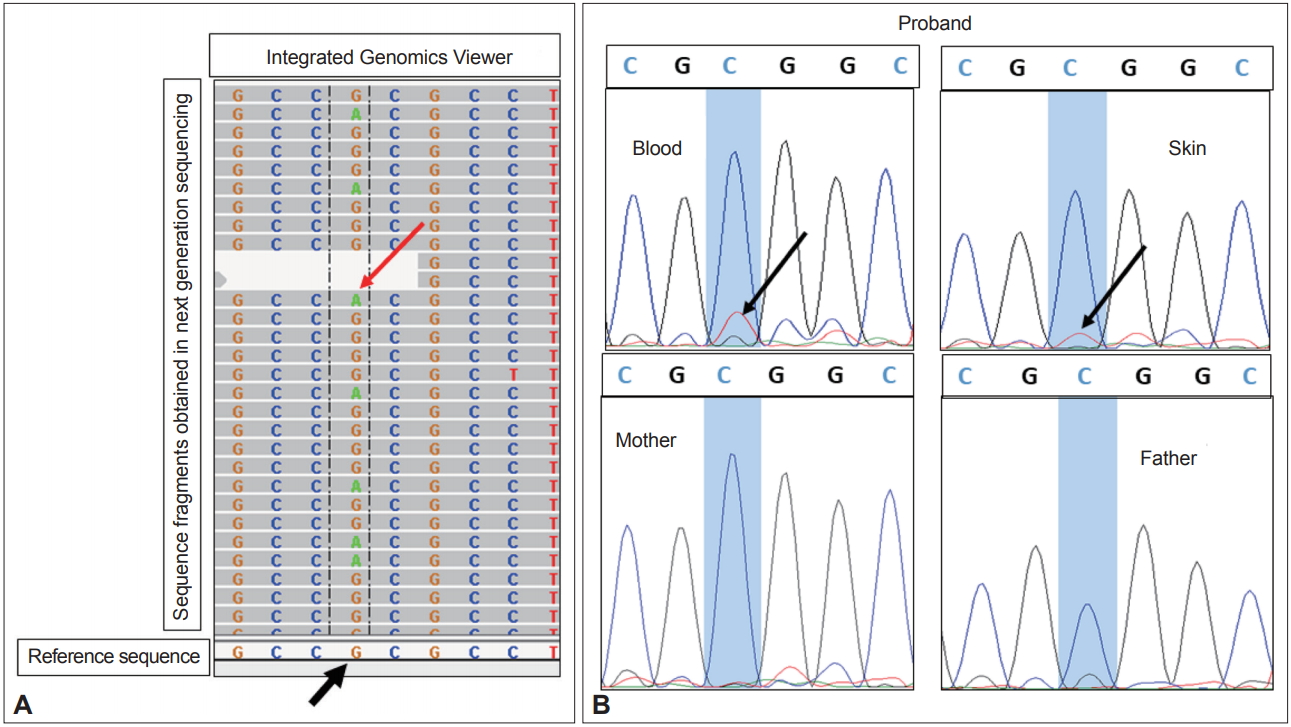
Exome and Sanger sequencing for p.R418W variant in ADCY5 gene. A: Sequences in Integrated Genomics Viewer (IGV) show mosaic variation c.1252C > T (since the gene is in reverse orientation, the variant seen is G > A). The reference sequence shows G (black arrow), and the multiple sequence fragments obtained by next generation sequencing show G in most of the reads and A (red arrow) in few reads, suggesting mosaicism for the G > A variation. B: Sanger sequencing of variant c.1252C > T shows a small peak of T allele (black arrows) in blood DNA and skin DNA in the proband, whereas both parents were shown to be homozygous for wildtype allele C.
Multiple medication treatments were attempted: clonazepam had mild benefit, and no benefit was observed with carbamazepine, tetrabenazine, propranolol, or trihexyphenidyl. The patient’s symptoms worsened on acetazolamide. Coffee therapy was also attempted in view of a recent report of a dramatic response. The patient was administered the coffee powder equivalent of approximately 100 mg of caffeine in two to three divided doses of coffee drink throughout the day in addition to a bedtime coffee drink. He subjectively reported 50–70% resolution of the nocturnal attacks with coffee therapy. Repeat video EEG showed 20 nocturnal dyskinetic events (each event lasting ~3 minutes). As the patient experienced gastric discomfort from the excessive coffee drink consumption, we tried treating him with caffeine capsules. The patient was given one capsule of 100 mg caffeine at bedtime while continuing 0.5 mg clonazepam at bedtime. The patient subjectively reported 90% reduction in attacks with a decrease in the severity of individual events from day one of treatment with the caffeine capsules. Video EEG conducted at 2 months after the initiation of coffee capsule treatment showed > 90% reduction in the number of attacks (only 3 events per night compared to 30 events per night prior to therapy) as well shortening of the attacks (event duration of around 1 minute post-therapy compared to 3 minutes prior to therapy) (Supplementary Video 3 in the online-only Data Supplement; patient testimonial). The patient showed a sustained response to therapy without any adverse effects at 3 month follow-up in January 2020.
Adenylyl cyclases are the family of enzymes that convert adenosine triphosphate to cyclic adenosine monophosphate (cAMP), the second messenger involved in a broad range of cellular activities. Adenylyl cyclase type V is the major isoform expressed in the brain (predominantly in the nucleus accumbens and striatum) and the heart. Monoallelic variations in ADCY5, causing gain of function and thus, excessive accumulation of cAMP, have been reported to cause hyperkinetic involuntary movements [6,7].
Since the first report of ADCY5 mutation-related dyskinesia in 2012, multiple cases have been reported across the globe [2]. Clinical presentations have varied depending on the type of mutation, environmental factors, background genes and the mosaic state of the mutation (mutant load). Patients with low mutation load, as occurs in somatic mosaicism, may manifest with milder clinical features in the form of purely paroxysmal involuntary movements in sleep, with normal interictal examination, as observed in our case [4].
A definitive consensus regarding the management of this condition has not been achieved, and no single drug has been found to be unequivocally beneficial. Various drugs have been used for the paroxysmal nocturnal involuntary movements, including acetazolamide, propranolol, clonazepam, clobazam, carbamazepine, tetrabenazine, trihexyphenidyl, and methylphenidate, with variable response. Paradoxically, some of these medications have been reported to worsen the symptoms, such as caffeine and tetrabenazine in one case each. Our patient noted worsening with acetazolamide and approximately 25% improvement with clonazepam. Video electroencephalography (VEEG) was used to record the burden of the attacks and showed 30 attacks with an average duration of approximately 3 minutes each, which constitutes marked sleep quality disturbance. One recent case report suggested a dramatic response to caffeine in a familial case [5]. The probable mechanism of action is reduction of cAMP production by caffeine.
This is the first Indian report of a mosaic common pathogenic variation in the ADCY5 gene causing purely nocturnal PxD, and it is the first case in which serial VEEG quantified dramatic improvement in nocturnal dyskinesia through caffeine therapy.
Awareness of the spectrum of this disease is important, as it can be mistaken for a seizure, psychogenic disorder or parasomnia. There is also a need to explore treatment options, as currently available medications have generated variable responses. Caffeine has shown some promise, but it needs to be tested more systematically and in a greater number of patients.
Supplementary Material
The online-only Data Supplement is available with this article at https://doi.org/10.14802/jmd.20014.
Video 1.
Event 1. Patient is initially drowsy, as noted by the drowsy pattern in EEG. This patient is noted to have arousal just before the onset of motor events, confirmed by posterior alpha rhythm on EEG. The motor event is characterized by generalized dyskinesia. The patient is awake and responsive during the event, as confirmed by the examiner in the video. Informed consent was obtained from patient for using his video (without masking) for publication purpose.
Video 2.
Event 2. Initial drowsy rhythm is followed by arousal just prior to the motor event, confirmed by posterior alpha rhythm. The motor event is characterized by generalized dyskinetic movements, with the patient being awake and responsive throughout the event, as confirmed by the examiner in the video. Informed consent was obtained from patient for using his video (without masking) for publication purpose.
Video 3.
Patient testimonial. This video depicts the patient’s testimonial. He states to the interviewer in his native south Indian language (with English subtitles) that his event frequency per night has been remarkably reduced from 20 to 2. The duration of each event has also been remarkably reduced from 3–5 minutes to less than 1 minute. Informed consent was obtained from patient for using his video (without masking) for publication purpose.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Ashwin Dalal, Gopal Krishna Dash. Data curation: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Meera Devan, Ashwin Dalal, Gopal Krishna Dash, Apuroopa Jannabhatla. Formal analysis: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Meera Devan, Ashwin Dalal, Gopal Krishna Dash, Apuroopa Jannabhatla. Investigation: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Meera Devan, Ashwin Dalal, Gopal Krishna Dash, Apuroopa Jannabhatla. Methodology: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Meera Devan, Ashwin Dalal, Gopal Krishna Dash, Apuroopa Jannabhatla. Project administration: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Ashwin Dalal, Gopal Krishna Dash. Resources: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Meera Devan, Ashwin Dalal, Gopal Krishna Dash, Apuroopa Jannabhatla. Supervision: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Ashwin Dalal, Gopal Krishna Dash. Validation: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Ashwin Dalal, Gopal Krishna Dash. Visualization: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Ashwin Dalal, Gopal Krishna Dash. Writing—original draft: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Meera Devan, Ashwin Dalal, Gopal Krishna Dash, Apuroopa Jannabhatla. Writing—review & editing: Kuldeep Shetty, Asodu Sandeep Sharma, Siddaramappa Jagadish Patil, Ashwin Dalal, Gopal Krishna Dash. Approval of final manuscript: all authors.
Acknowledgements
The authors are thankful to the family for participation in the study.