The Impact of Impulsivity on Quality of Life in Early Drug-Naïve Parkinson’s Disease Patients
Article information

Abstract
Objective
Impulse control disorders (ICDs) in Parkinson’s disease (PD) are mostly related to dopamine replacement therapy (DRT); however, drug-naïve PD patients have also frequently experienced impulsivity. This phenomenon makes clinicians hesitate treating patients with DRT. In this study, we assessed the effect of impulsivity on quality of life (QOL) in drug-naïve PD patients.
Methods
Two hundred three newly diagnosed, nonmedicated PD patients were enrolled, and they received structured clinical interviews, physical examinations and validated questionnaires to evaluate motor and nonmotor symptoms and QOL. Impulsivity was evaluated using the Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale (QUIP-RS).
Results
Thirty-eight patients (18.7%) had impulsivity with QUIP-RS scores ≥ 1 and 4 patients (2.0%) were diagnosed with combined ICDs. Motor and nonmotor symptoms were significantly correlated with the Parkinson’s Disease Questionnaire-39 summary index. Female sex and QUIP-RS scores were also correlated with QOL in drug-naïve PD patients.
Conclusion
The results of the present study showed that impulsivity negatively influences QOL in early drug-naïve PD patients. In addition, more severe motor and nonmotor symptoms were also associated with lower QOL. Such findings complicate treatment but provide valuable information for managing early PD.
Parkinson’s disease (PD) is a multisystem disorder with progressive degeneration of the nigrostriatal dopaminergic systems and widespread extranigral pathology affecting different anatomical structures and neurotransmitters. Dopamine replacement therapy (DRT) is regarded as an effective strategy for the management of motor and nonmotor symptoms in PD; however, this treatment is associated with motor and behavioral adverse effects, such as levodopa-induced dyskinesia, motor fluctuation and impulse control disorders (ICDs). The development of DRT-related adverse effects is associated with the dosage and duration of the dopaminergic medications [1]. Therefore, dose reduction or discontinuation of dopaminergic medication is still the most effective therapy for these adverse effects. However, the aggravation of motor symptoms or the occurrence of a withdrawal syndrome presents an awkward dilemma to clinical practitioners.
The ICDs are defined by a failure to resist an impulse that causes harm to people. These include pathological gambling, hypersexuality, binge eating and compulsive shopping. An increased frequency of ICDs has been associated with the use of dopaminergic drugs in patients with PD. In particular, the use of dopamine agonists, which have high affinity for the D3 receptor, has been known to be the most reliable contributor to ICD [2]. However, some drug-naïve patients with PD also have ICDs [3]. Furthermore, PD patients who received dopamine agonists usually showed a higher prevalence of ICD than restless leg syndrome patients with dopamine agonist treatment [4]. Therefore, although the prevalence could be affected by personality traits, it has also been supposed that PD pathology may influence the development of ICDs.
Impulsivity has a broad definition in psychiatry and has not been clearly defined. Impulsivity is understood to be a multidimensional construct involving aspects such as impulsive choice and impulsive traits. ICD patients are considered more impulsive than healthy individuals. PD patients without ICD can exhibit characteristics of increased impulsivity and therefore might be at greater risk for developing an ICD than normal subjects [5,6]. Because ICDs can cause serious physical, psychological and social problems or distress for the patients as well as caregivers, clinicians may hesitate increasing dopaminergic medication in cases of need. In particular, drug-naïve PD patients who have experienced uncontrolled impulsivity or reward-seeking problems have a limit on the treatment of their motor symptoms.
The hypothesis tested in this study was that impulsivity in the de novo state affects various clinical aspects of motor and nonmotor features and quality of life (QOL) in early PD. In the present study, we investigated the influence of impulsivity on motor and nonmotor symptoms in drug-naïve PD patients and assessed the association of impulsivity with QOL to develop better treatment strategies in drug-naïve PD patients with impulsivity.
MATERIALS & METHODS
Patients
The study protocol was approved by the Institutional Review Board of our institution (IRB No. KC17ONSI0423), and all subjects provided written informed consent to participate. All experiments were performed in accordance with the relevant guidelines and regulations.
Newly diagnosed, early PD patients who visited the movement disorder clinic at the tertiary university hospital between May 2016 and December 2017 were enrolled. They were diagnosed with PD according to the criteria of the UK PD Society Brain Bank [7]. Their clinical diagnosis was substantiated by positron emission tomography using 18F-N-(3-fluoropropyl)-2beta-carbon ethoxy-3beta-(4-iodophenyl) nortropane imaging; all patients had presynaptic dopamine transporter uptake deficiency in the striatum. Patients who had other medical problems that caused serious disability, such as severe dementia, stroke, cardiovascular disease, blindness, deafness and osteoarthritis, were excluded.
Clinical assessment
Clinical information was obtained for age, sex, body mass index (BMI), disease duration, familial history of PD, history of arterial hypertension, diabetes mellitus and cigarette smoking. The United Parkinson Disease Rating Scale (UPDRS), modified Hoehn and Yahr stage (H&Y) and nonmotor symptoms scale (NMSS) were evaluated in all enrolled subjects [8-10]. Cognitive function and dementia severity were evaluated with the Korean Mini-Mental State Examination (K-MMSE) and Clinical Dementia Rating (CDR) [11,12].
Impulsivity was assessed by the Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease-Rating Scale (QUIP-RS), which consisted of questions about impulsivity related to gambling, sexuality, eating, buying, hobbyism and punding behaviors and dopamine medication use [13]. Subjects were considered to have an ICD if their QUIP-RS was ≥ 10, and this cutoff value had been previously validated [13]. The presence of impulsivity was defined by a questionnaire-based assessment, and we regarded a QUIP-RS of more than 1 as a subject with impulsivity. QOL of the enrolled subjects was evaluated with the Parkinson’s Disease Questionnaire-39 (PDQ-39), which consisted of 8 domains about mobility, activities of daily living (ADLs), emotion, stigma, social, cognition, communication and bodily discomfort [14]. Higher scores on the PDQ-39 indicated poorer QOL. All questionnaires were evaluated blind to the clinical information of the patients.
Statistical analysis
All statistical analyses were conducted with SPSS software version 24.0 for Windows (IBM Corp., Armonk, NY, USA). Independent sample t-tests were used to compare group-mean differences, and Pearson’s χ2 tests were used to compare frequencies for categorical variables. The association of the PDQ-39 scores with clinical and demographic data, as well as impulsivity, was assessed using Spearman’s correlation coefficients. A multiple linear regression analysis was performed with the PDQ-39 score as a dependent variable and age, sex, BMI, hypertension, diabetes mellitus, smoking status, disease duration, family history of PD, UPDRS part III score, NMSS score and QUIP-RS score as covariates. Independent variables were selected based on a model in a previous study and on theoretical grounds [15]. Statistical significance was set at p < 0.05.
RESULTS
A total of 203 drug-naïve, de novo PD patients were included in this study; the mean age was 69.3 ± 0.7 years, and 97 patients were male (47.8%). Thirty-eight patients (18.7%) had impulsivity with a QUIP-RS score ≥ 1, and the overall mean score in the group with impulsivity was 4.7 ± 5.2 points on the QUIP-RS. Four patients were diagnosed with combined ICD, and there were 2 pathological gambling (1.0%), 1 compulsive shopping (0.5%), and 1 binge eating (0.5%) patients. One patient had hobbyism and punding (0.5%).
The clinical characteristics between the groups with impulsivity and without impulsivity are shown in Table 1. PD patients with impulsivity had a more frequent family history of PD and higher NMSS score than those without impulsivity. There were no significant differences in the other clinical characteristics, including UPDRS, H&Y, K-MMSE and CDR measures.
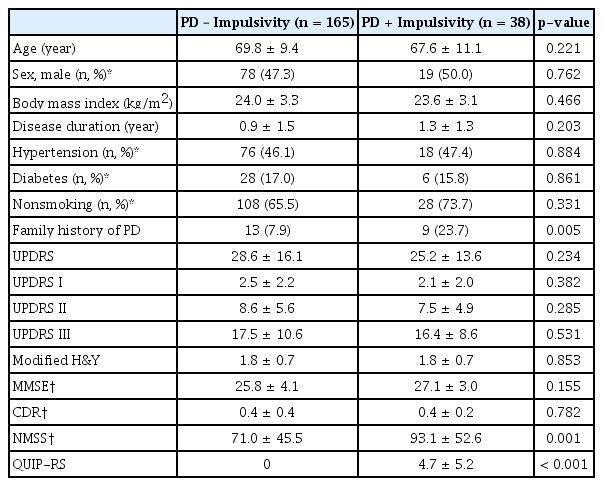
Clinical characteristics of the subjects
The comparison of QOL between the patients with impulsivity and those without impulsivity is shown in Table 2. The PDQ-39 summary index and subdomain scores, such as mobility, ADLs, emotional well-being and bodily discomfort, were higher in patients with impulsivity than in those without impulsivity. However, stigma, social support, cognition, and communication domains were not significantly different between the patient groups.
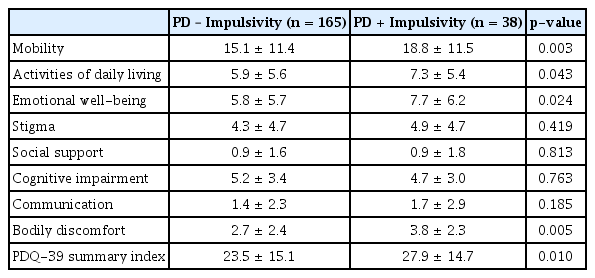
Comparison of QOL (8 domains of PDQ-39) between participants with impulsivity and without impulsivity
The correlation test results between demographic factors, NMSS, UPDRS part III motor score and QUIP-RS measures and the PDQ-39 summary index are summarized in Table 3. Female sex (β = 3.462), BMI (β = 0.534), UPDRS part III motor score (β = 0.336), NMSS score (β = 0.212) and QUIP-RS score (β = 0.453) were significantly correlated with the PDQ-39 summary index, and disease duration showed a borderline significant trend (β = 0.759). This model explained 67.4% of the variance in the PDQ-39 summary index, which was statistically significant (F = 35.967, p < 0.001).

Association of demographic factors, motor and nonmotor symptom scores and QUIP-RS scores with the PDQ39 summary index
DISCUSSION
Impulsivity was relatively commonly found among the patients in this study. The impulsivity was associated with increasing NMSS scores in early drug-naïve PD patients. In addition, impulsivity was related to higher levels of a poor QOL in these patients. PD patients with impulsivity more frequently had a family history of PD. It is supposed that genetic factors could be related to impulsivity. However, the number of PD patients, especially those with a familial history of PD, was too small for generalization.
PD patients with an ICD have a poorer QOL than those without an ICD [16]. Our results also found that PD patients with impulsivity showed a tendency to have a poorer QOL than PD patients without impulsivity. This finding is consistent with an earlier report showing that ICD frequently occurred in de novo PD patients [3]. However, the degree of effect associated with the presence of an ICD contributing to an overall poorer quality across aspects of their lives was smaller and less significant than the degree of effect associated with the motor symptoms or nonmotor symptoms. This finding may be mainly due to more severe nonmotor symptoms in PD patients with impulsivity. These findings corresponded well with those in an earlier study, which demonstrated that nonmotor symptoms significantly affected QOL in early PD patients [17]. Considering that nonmotor symptoms as well as motor symptoms could be improved by dopaminergic treatment, sufficient treatment may be a better choice to enhance QOL in PD patients who have some impulsivity.
From our analysis, the patients’ QOL was affected by nonmotor symptoms. Nonmotor symptoms affected QOL more than motor symptoms did. In addition, female PD patients showed lower QOL than male patients. The sex differences in nonmotor symptoms have been widely investigated [18], and it has been considered that socioeconomic status, occupational functioning, and hormonal differences between the sexes could contribute to these differences. This finding is in line with current published evidence that practitioners should be concerned with managing nonmotor symptoms as well as motor symptoms in de novo PD patients [19].
In the present study, the prevalence of combined ICD was 2.0%, which is lower than reported by other studies [3]. This may have been caused by two factors. One factor is that our study was conducted in drug-naïve PD patients. ICDs have been more frequently reported in levodopa-medicated PD patients receiving higher doses of DRT, especially D3 dopamine agonists. Furthermore, the distinct characteristics of the place and culture in which the present study was conducted may be another cause. Presenting a desire for sexuality, gambling and possessions are taboo in the Confucian culture of Korea. The differences in race and medical service systems may also have affected this low prevalence of ICD. In Korean PD patients, a previous study had demonstrated that the prevalence of ICD was 1.3% for gambling, 2.8% for hypersexuality, 2.5% for pathological shopping and 3.4% for binge eating, which were also lower than the prevalence reported in other countries [20].
Although ICDs were infrequent in the present study, 18.7% of de novo PD patients experienced impulsivity. Without the effects of DRT, nigrostriatal degeneration and decreased dopamine reuptake may be another cause of ICD. Lower dopamine transporter availability in drug-naïve PD patients was associated with the subsequent development of an ICD after DRT [21]. Problems of impulsivity, decision making or the reward system would easily be predicted based on those anatomical and physiological changes [22]. It is supposed that ICDs may become more likely after DRT on the basis of PD pathology. Continuity theory, which asserts that most PD patients are affected to some degree with impulsivity problems, has been addressed in recent years [3].
Though QOL was affected by ICDs in the PD patients, it was less impactful than other neuropsychiatric symptoms in earlier reports [15]. Hypodopaminergic disorders, such as depression, anxiety or apathy, have larger detrimental effects on QOL than hyperdopaminergic symptoms [23]. Hobbyism, which is an impulse control related disorder, was negatively correlated with poor QOL in PD patients in a recent study. Excluding some antisocial behaviors related to hypersexuality or pathological gambling, ICDs may be less likely to be a major problem for PD patients in comparison with hypodopaminergic motor and nonmotor symptoms.
The limitations of our study are as follows. First, a diagnosis of PD was determined with clinical diagnostic criteria rather than with neuropathological confirmation. Second, as previously described, the number of PD patients with an ICD was small in our sample, and therefore care should be taken when interpreting the results of this study. Though our findings in the present study show similarity to previous studies, a larger study for comparison would be needed. Third, we did not use the Barratt impulsivity scale, which is one of the tools evaluating self-reported impulsivity. The QUIP-RS was developed to screen and assess the severity of ICDs and has sometimes been used as a measure of impulsivity [24]. Though QUIP-RS is not usually used for measuring impulsivity, we supposed that QUIP-RS could represent some aspects of impulsivity. Fourth, no age-matched healthy controls were involved in this study. Finally, all the factors related to QOL could not be analyzed within our statistical analysis. However, our regression model showed a high coefficient of determination, which is an indication of how well the predictions approximated the actual data.
In summary, we found an association between impulsivity and QOL in drug-naïve de novo PD patients. In addition, impulsivity was associated with motor and nonmotor symptoms. Such findings complicate treatment but provide valuable information for managing early PD.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Acknowledgements
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (NRF-2017R1D1A1B06028086).