Musculoskeletal Problems Affect the Quality of Life of Patients with Parkinson’s Disease
Article information

Abstract
Objective
Musculoskeletal problems are more common in patients with Parkinson’s disease (PD) than in normal elderly, but the impact of musculoskeletal problems on health-related quality of life (HRQoL) in patients with PD is unknown.
Methods
Four hundred consecutive patients with PD were enrolled for the evaluation of musculoskeletal problems and HRQoL. HRQoL was assessed by the 36-Item Short Form Health Survey, which comprised physical health and mental health.
Results
Of the total patients, 265 patients had musculoskeletal problems, and 135 patients did not have musculoskeletal problems. Patients with musculoskeletal problems reported lower levels of HRQoL in terms of physical health than did patients without musculoskeletal problems (p < 0.05). In women, all components of physical health were lower in patients with musculoskeletal problems than in patients without musculoskeletal problems (p < 0.05). Meanwhile, in men, only the bodily pain score of physical health was lower in patients with musculoskeletal problems than in patients without musculoskeletal problems. Mental health and physical health were negatively correlated with depression, Unified Parkinson’s Disease Rating Scale I & II scores, and pain severity from musculoskeletal problems, in that order (p < 0.01 for all).
Conclusion
These results suggest that musculoskeletal problems in patients with PD affect HRQoL significantly, mainly in terms of physical health rather than mental health and especially in women rather than men. Musculoskeletal problems should not be overlooked in the care of patients with PD.
Musculoskeletal problems are very common (45–66.3%) in patients with Parkinson’s disease (PD) [1,2]. However, there is limited evidence for the impact of musculoskeletal problems on quality of life (QoL) in patients with PD [3]. One paper evaluating 48 PD patients reported that bradykinesia and musculoskeletal impairments are correlated with life satisfaction [4]. Andreadou et al2 reported that even though musculoskeletal problems are the most common comorbidity in patients with PD, depression is more of a contributing factor to QoL than are musculoskeletal problems in patients with PD [2]. In our previous paper evaluating musculoskeletal problems in patients with PD, 31.8% (83/263) of PD patients with musculoskeletal problems responded that musculoskeletal problems limited their activity of daily living more than did the PD symptoms [1].
Musculoskeletal problems are known to be the most common cause of physical disability in the general population [5]. In addition, musculoskeletal disorders have been associated with the largest losses of QoL in the general population [6]. Because PD usually develops in old age and has a long disease duration, musculoskeletal problems in patients with PD could be an important issue that cannot be ignored [7].
In this study, we estimated the impact of musculoskeletal problems on health-related QoL (HRQoL) in patients with PD, focusing on the following questions.
1) Do musculoskeletal problems affect HRQoL in PD patients? Which components among HRQoL are mainly affected?
2) What types of clinical characteristics affect musculoskeletal problems in PD patients?
MATERIALS & METHODS
Subjects
This study was designed as a cross-sectional evaluation of musculoskeletal problems in 400 patients with PD. All subjects were from the PD cohort of the Movement Disorder Clinic of Seoul National University Hospital: 265 patients with musculoskeletal problems and 135 patients without musculoskeletal problems. Details of the case-finding procedures and other characteristics of the musculoskeletal problems have been published elsewhere [1]. Briefly, patients were enrolled consecutively in an outpatient clinic from October 2011 to June 2012, and their musculoskeletal problems were evaluated. Patients with atypical parkinsonism were excluded. Patients with severe cognitive or speech problems who could not explain their symptoms were excluded. This study was approved by the Institutional Review of Board at Seoul National University Hospital. Written informed consent was obtained from all participants.
Clinical assessments
Physicians interviewed all patients using a structured format. During the interview for the musculoskeletal problems, the following relevant evaluations, including the 36-Item Short Form Health Survey (SF-36), were performed at the same time.
1) Musculoskeletal problems are linked anatomically by their association with pain or impaired physical function [8]. The existence of current musculoskeletal problems was discriminated according to the criteria we described in our previous study [1]. In addition, pain intensity (using a visual analog scale, VAS) related to musculoskeletal problems was evaluated.
2) Demographic factors included sex, age, age at onset, PD duration, the Unified Parkinson’s Disease Rating Scale (UPDRS) scores, the Hoehn and Yahr (HY) stage, and the levodopa equivalent daily dose [9].
3) The Beck Depression Inventory (BDI), a selfreported questionnaire, was used to measure the severity of depression.
4) HRQoL was assessed with the SF-36 questionnaire, which is a validated questionnaire comprising 36 questions. SF-36 is mainly divided into 2 categories of physical health and mental health. Physical health and mental health are composed of 4 dimensions each; physical health includes physical functioning, role-physical, bodily pain and general health, and mental health comprises vitality, social functioning, role-emotion, and mental health (range 0–100, higher scores indicate a better health status) [10].
Statistical assessments
In the case of continuous variables, the differences in HRQoL or other demographic features according to the existence of musculoskeletal problems were evaluated by independent t-tests. Noncontinuous variables were compared by chi-squared tests. To analyze the true effect of the MS problem on HRQoL (SF-36), other covariates that are not of primary interest were adjusted for by analysis of covariance. In addition, the relationships between the pain severity from musculoskeletal problems and HRQoL, BDI, and other clinical factors were calculated with Pearson’s correlation coefficients. A p value of < 0.05 was considered significant in all tests. These statistical analyses were performed with IBM SPSS statistics software ver. 19.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The clinical profiles of the PD cohort are summarized in Table 1, and all data except for the BDI scores were already published in our previous paper [1]. Women, older age, older onset of PD, a higher UPDRS part I and II summed score, and a higher BDI score were associated with the existence of musculoskeletal problems in PD (Table 1). To evaluate HRQoL between the groups with and without musculoskeletal problems, the SF-36 score was adjusted by these significant contributing factors. Patients with musculoskeletal problems reported lower levels of QoL in terms of physical functioning, bodily pain, and general health (p = 0.003, p < 0.001, and p = 0.013, respectively) than did patients without musculoskeletal problems. Physical health, which is the mean score of physical functioning, role-physical, bodily pain, and general health, was also lower in patients with musculoskeletal problems than in patients without musculoskeletal problems (p = 0.003). However, mental health scores were not different between the groups (Table 1).
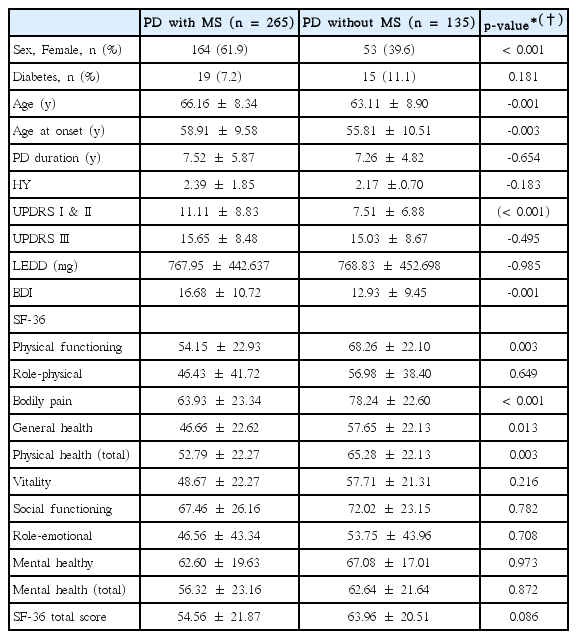
Comparison of quality of life, sleep adjusted by sex, age, age at onset, UPDRS scores, and depression scores in all patients
In women, the BDI score was the only factor that was different between patients with and without musculoskeletal problems (p = 0.022). After adjusting for the BDI score, all the components of physical health were lower in patients with musculoskeletal problems than in patients without musculoskeletal problems (p < 0.05 for all). Mental health was not different between the groups (Table 2). In men, older age, older age at onset, and higher UPDRS I & II scores were significantly associated with musculoskeletal problems (p = 0.001, p = 0.001, and p < 0.001, respectively). All subscores of the SF-36 except for bodily pain were not different between the groups after adjusting for age, age at onset, and UPDRS I & II scores (Table 3).
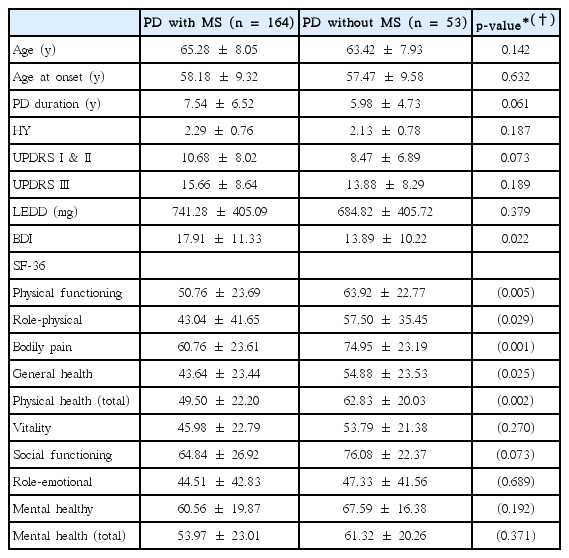
Comparison of quality of life adjusted by BDI score based on the existence of musculoskeletal problems in women
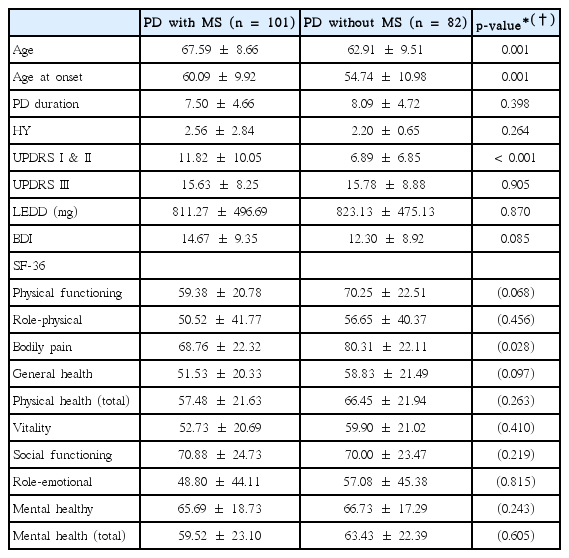
Comparison of quality of life adjusted by age, age at onset, and UPDRS scores based on the existence of musculoskeletal problem in men
In the correlation analysis between HRQoL and associated factors, mental health and physical health were more negatively correlated with the BDI score, UPDRS I & II scores, and pain severity from musculoskeletal problems, in that order (p < 0.01) (Table 4).

Pearson’s correlation coefficients between various factors
DISCUSSION
The present study has three main findings. First, musculoskeletal problems in PD affect HRQoL significantly, mainly in terms of physical health. Second, musculoskeletal problems in PD have different effects on QoL according to gender. Third, musculoskeletal problems as well as depression and UPDRS I & II are important factors associated with HRQoL in PD.
The existence of musculoskeletal problems in PD contributed to a poor QoL in terms of physical health. Regarding mental health, the existence of musculoskeletal problems did not have an impact on QoL. Although the UPDRS motor score and HY stage were not different based on the existence of musculoskeletal problems, HRQoL was poor regarding musculoskeletal problems even after adjusting for other factors, including UPDRS part I and II scores and age. In the general population, musculoskeletal problems are associated with the largest losses of QoL [6]. However, in PD, our study suggested that musculoskeletal problems were associated with a poor QoL in terms of physical health, although this association was weaker than the associations of PD symptoms or depression with a poor QoL.
Musculoskeletal problems are more common in women than in men and have more significant contributions to QoL in women than in men in terms of physical health. All components of physical health in women and bodily pain in men affected QoL by musculoskeletal problems in PD. Women are at a higher risk than men for musculoskeletal problems in the general population [8]. In addition, women reported neck and low back pain more frequently than men at the onset of PD [11]. However, it is difficult to know whether this is because of the difference in pain severity in men and women. In this study, the pain severity from musculoskeletal problems was not different between men and women (pain severity assessed by VAS score; median values were 1 and 2, and the means with SD were 1.79 ± 2.20 and 2.01 ± 2.23 in women and men, respectively, p = 0.347). Women with PD could be more susceptible to musculoskeletal problems than men with PD, which would have a greater impact on QoL.
Patients with musculoskeletal problems had higher depression scores than patients without musculoskeletal problems, and this was more prominent in the female population. In addition, depression was well correlated with pain severity from musculoskeletal problems. Musculoskeletal problems in PD may contribute, even partially, to depression. Another aspect was that depression was negatively correlated with QoL in both physical health and mental health categories. It was already reported that depression is the most consistent determinant affecting QoL in PD [2,12]. In this study, a higher depression score was strongly correlated with a lower QoL score. Depression, compared to other factors, was a more important factor contributing to HRQoL in patients with PD.
The strength of the present study is its relatively large PD sample. In addition, this is the first assessment of the impact of musculoskeletal problems on the QoL in patients with PD. This study has some limitations. First, musculoskeletal problems were assessed by physical examination and interview. Structured assessment tools such as imaging were not used, and experts in the field of musculoskeletal problems were not involved in the study. Second, this was a cross-sectional evaluation and did not include any longitudinal clinical outcomes.
In conclusion, musculoskeletal problems in PD affect HRQoL significantly, mainly in terms of physical health rather than mental health and especially in women rather than in men. Musculoskeletal problems should not be overlooked in the care of patients with PD.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Acknowledgements
This study was supported by a grant from the Korea Health Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (A101273).