Letter to the editor Wall-Eyed Bilateral Internuclear Ophthalmoplegia Syndrome in a Patient With Progressive Supranuclear Palsy: A Case Report and Literature Review
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Patients with progressive supranuclear palsy (PSP) present features including vertical gaze palsy, pseudobulbar palsy, dysarthria, axial rigidity, and dementia. In the revised clinical diagnostic criteria of PSP of the Movement Disorders Society, ocular motor dysfunction was proposed as one of the four core functional domains [1]. Ocular motor dysfunction includes three main features: O1) vertical supranuclear gaze palsy, O2) slow velocity of vertical saccades, and O3) frequent macro square wave jerks or “eyelid opening apraxia”. There have been several case reports of wall-eyed bilateral internuclear ophthalmoplegia (WEBINO) in patients with PSP (Supplementary Table 1 in the online-only Data Supplement). However, WEBINO has not yet been established as a clinical feature in patients with PSP. Herein, we report a case of PSP with WEBINO and review previous case reports.
A 63-year-old man came to the clinic with dysphonia and bradykinesia. He had developed a husky voice and slow gait 4 months prior. He reported getting slower when taking a shower and occasionally experienced drooling. He denied having rapid eye movement sleep behavior disorder, constipation, or voiding difficulties. He had experienced a small left cerebellar infarction, which occurred 1 year prior, and reported hypertension, gout, and asthma. On neurological examination, he showed a masked face and mild bradykinesia in the left hand. 18F-N-(3-fluoropropyl)-2β-carboxymethoxy-3β-(4-iodophenyl) nortropane (18F-FP-CIT) positron emission tomography (PET) showed decreased uptake in the bilateral basal ganglia (Figure 1), which was worse on the right side. There was no evidence of Parkinson-plus syndrome on the initial brain magnetic resonance imaging (MRI) scan. We started levodopa to control his parkinsonism, which worked for several months. However, the response became poor despite a dose increase of up to 450 mg per day. He complained of postural instability with a relatively rapid progression in the last 3 years.
On a subsequent visit, 4 years after the initial presentation, the patient developed horizontal diplopia, especially while looking at the close objects. His eyes showed bilateral exotropia in the primary eye position and vertical gaze limitations (Figure 1). Spontaneous saccadic intrusions were present, which increased without fixation (Supplementary Figure 1 in the online-only Data Supplement). In his horizontal gaze, an adduction deficit with abducting nystagmus was shown, which was compatible with WEBINO syndrome (Supplementary Video 1 in the online-only Data Supplement). Convergence was impaired, while the oculocephalic response was preserved, which was confirmed by a video-assisted head impulse test.
He also had frequent blepharospasm. We reconsidered his clinical manifestations and tried to find another cause of WEBINO. He did not have autonomic dysfunction, such as urinary retention, severe orthostatic hypotension or cerebellar ataxia. Follow-up brain MRI revealed severe atrophy of the midbrain (Figure 1) and no other new intra-axial brain lesions contributing to WEBINO. We increased the levodopa dose to 600 mg per day for 6 months, but it was not effective. The patient was barely able to walk with a cane and experienced frequent falls more than once a day, which was compatible with a Hoehn and Yahr stage 4 rating.
Until the development of WEBINO and vertical gaze limitations, the patient could have been diagnosed with suggestive PSP with predominant parkinsonism (A2 + CC1). However, he ultimately satisfied the clinical criteria for probable Richardson’s syndrome (PSP-RS) [1]. His core clinical features, including O1 (vertical supranuclear gaze palsy) and A2 (parkinsonism, akinetic-rigid, predominantly axial, and levodopa-resistant), confirmed the final diagnosis [2].
WEBINO in the clinical course of PSP can make diagnosis challenging. This patient was diagnosed with PSP-RS based on his asymmetric parkinsonism with poor response to levodopa, early postural instability, and neuro-ophthalmologic findings [1].
WEBINO consists of primary gaze exotropia, bilateral adduction impairment, and abducting nystagmus in both eyes. WEBINO syndrome has been reported in patients with brainstem infarction, tumor, multiple sclerosis, infection, head trauma, inflammation, poor nutrition (Wernicke’s encephalopathy or pernicious anemia), toxic/metabolic conditions, and congenital malformation (Arnold-Chiari malformation). These conditions result in disturbance of the bilateral medial longitudinal fasciculus (MLF) [3]. The MLF carries signals for horizontal conjugation from the abducens nucleus to the contralateral medial rectus subnucleus of the oculomotor nerve. Weakening of the medial rectus muscle due to MLF lesions prompts the higher oculomotor centers to increase innervation to the medial rectus to compensate for the paresis. The contralateral lateral rectus also receives additional innervation as the corresponding synergist muscle, resulting in abducting nystagmus. However, the cause of primary gaze exotropia in WEBINO is still controversial. On neuroimaging studies, WEBINO is not necessarily pontine in origin, and the responsible lesion can extend into the midbrain as well [4]. Other studies have claimed that small subgroups of medial rectus neurons embedded within the MLF are responsible for exotropia, leaving the oculomotor nerve nucleus intact [5]. Some studies have reported that the paramedian pontine reticular formation is also functionally involved in exotropia in patients with WEBINO syndrome.
There have been eight case reports of WEBINO in patients with PSP (Supplementary Table 1 in the online-only Data Supplement). Disease duration at the onset of WEBINO varies by case. Two cases showed WEBINO in the progressive course of PSP, as in our case, but not on initial examination. This difference might be attributed to tau burdens and cell-type-specific distribution patterns in the different clinical subtypes of PSP. In a recent study of distribution patterns of tau pathology in patients with PSP, significant differences in the tau burden as well as tau cytopathology distinguished the clinical subtypes [6]. Patients with PSP-P usually showed less total tau accumulation in the neocortical regions, selected subcortical regions, and brainstem nuclei than those with PSP with corticobasal syndrome (PSP-CBS) and PSP with predominant speech and language disorder (PSP-SL) [6]. According to the staging scheme in that study, common early vulnerability patterns mainly affecting the pallido-nigro-luysian axis characterize all PSP clinical subtypes. Subsequently, tau pathology propagates rostrally to neocortical regions and caudally to the cerebellum, including the dentate nucleus. The development of WEBINO in this patient after initial parkinsonism without significant cortical symptoms implies that tau pathology progressed caudally and impaired conjugated eye movements of the MLF bilaterally.
In summary, WEBINO should be considered as an oculomotor dysfunction in patients with PSP that can develop in the progressive course of the disease. WEBINO is not present in patients with other Parkinson syndromes, which suggests that it is a clinical indication of PSP in the differential diagnosis of parkinsonism.
Video-oculography showing spontaneous eye movements according to the existence of fixation (A, with fixation, B, without fixation). Video-oculography demonstrated the spontaneous salvos of abducting saccades followed by a drift of the abducting eye, with a decreasing velocity waveform, toward the initial position, and the adducting eye showed also a slow, small amplitude movement followed by a slower return to the initial ocular position. These saccadic intrusions (saccadic pulse trains) increased without fixation.
Ocular motor findings of the patient four years after the initial presentation. His eyes show bilateral exotropia in the primary eye position (00:00). Spontaneous saccadic intrusions are present, which increase without fixation (00:12). Adduction deficits with abducting nystagmus of both eyes are shown during bilateral horizontal gaze, which is compatible with WEBINO syndrome (00:25). Finally, there are vertical gaze limitations (00:49). WEBINO, wall-eyed bilateral internuclear ophthalmoplegia.
Notes
Ethics Statement
This report was approved by the Institutional Review Board of the Chungbuk National University Hospital (IRB File No. 2021-10-026-001), and the requirement of informed consent was waived.
Conflicts of Interest
The authors have no financial conflicts of interest.
Funding Statement
None
Author Contributions
Conceptualization: Aryun Kim, Chaewon Shin. Data curation: Yu Jin Jung. Investigation: Aryun Kim, Dallah Yoo. Methodology: Aryun Kim, Chaewon Shin. Supervision: Chaewon Shin. Visualization: Chaewon Shin, Seong-Hae Jeong. Writing—original draft: Aryun Kim. Writing—review & editing: all authors.
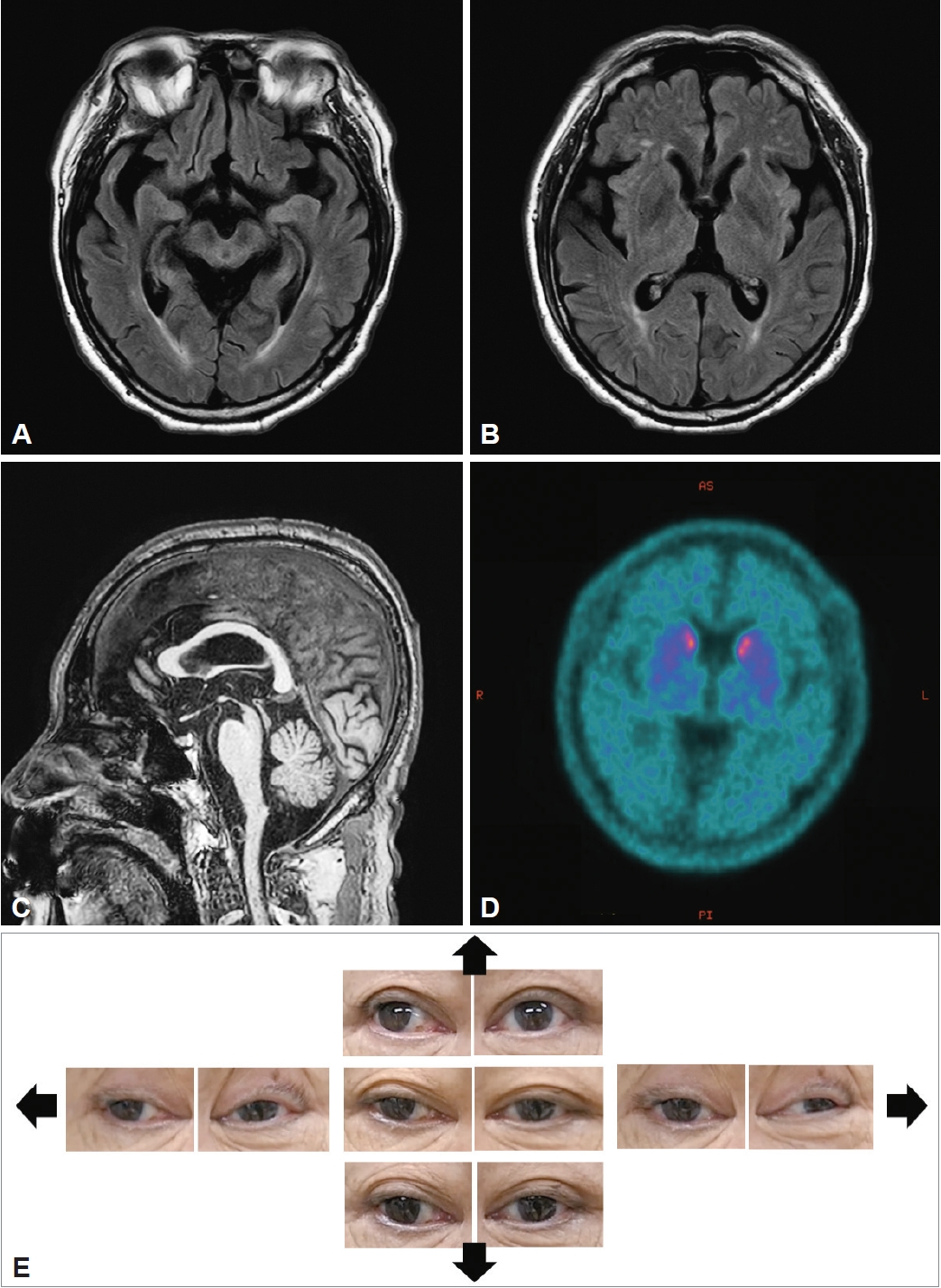
Figure 1.
Neuroimaging findings of the patient. A: Marked midbrain atrophy and medial and anterior temporal lobe atrophy are seen in the axial view of the brain MRI scan, which was taken 6 years after onset. B: There are no abnormal findings in the basal ganglia and high frontal and parietal cortices. C: The “humming bird sign” is seen on the sagittal view. D: 18F-FP-CIT PET shows severely decreased dopamine transporter uptake in the bilateral basal ganglia. E: Photographs of oculomotor abnormalities in the index case. Gaze positions: primary position, lateral (left and right arrow), upward (upper arrow), and downward (lower arrow). 18F-FP-CIT, 18F-N-(3-fluoropropyl)-2β-carboxymethoxy-3β-(4-iodophenyl) nortropane; PET, positron emission tomography; MRI, magnetic resonance imaging.
REFERENCES
1. Höglinger GU, Respondek G, Stamelou M, Kurz C, Josephs KA, Lang AE, et al. Clinical diagnosis of progressive supranuclear palsy: the movement disorder society criteria. Mov Disord 2017;32:853–864.ArticlePubMedPMCPDF
2. Grimm MJ, Respondek G, Stamelou M, Arzberger T, Ferguson L, Gelpi E, et al. How to apply the movement disorder society criteria for diagnosis of progressive supranuclear palsy. Mov Disord 2019;34:1228–1232.ArticlePubMedPMCPDF
3. Wu YT, Cafiero-Chin M, Marques C. Wall-eyed bilateral internuclear ophthalmoplegia: review of pathogenesis, diagnosis, prognosis and management. Clin Exp Optom 2015;98:25–30.ArticlePubMed
4. Chen CM, Lin SH. Wall-eyed bilateral internuclear ophthalmoplegia from lesions at different levels in the brainstem. J Neuroophthalmol 2007;27:9–15.ArticlePubMed
5. Glicksman MA. Localization of motoneurons controlling the extraocular muscles of the rat. Brain Res 1980;188:53–62.ArticlePubMed
6. Kovacs GG, Lukic MJ, Irwin DJ, Arzberger T, Respondek G, Lee EB, et al. Distribution patterns of tau pathology in progressive supranuclear palsy. Acta Neuropathol 2020;140:99–119.ArticlePubMedPMCPDF
 E-submission
E-submission
 , Yu Jin Jung2
, Yu Jin Jung2

 PubReader
PubReader ePub Link
ePub Link Cite
Cite
