Department of Neurology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Corresponding author: Sun Ju Chung, MD, PhD Department of Neurology, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea / Tel: +82-2-3010-3440 / Fax: +82-2-474-4691 / E-mail: sjchung@amc.seoul.kr
• Received: August 18, 2021 • Revised: September 17, 2021 • Accepted: September 27, 2021
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Dystonia is characterized by hyperkinetic movements with sustained muscle contractions, repetitive movements, and abnormal posturing of body parts [1]. Primary dystonia is considered a disorder of the basal ganglia in the brain, whereas secondary dystonia is caused by anatomical lesions in the brain [1]. Diagnosing dystonia is occasionally difficult because a condition that mimics dystonia, pseudodystonia, is also characterized by a wide spectrum of abnormal muscle contractions. Pseudodystonia may be caused by various neurological diseases that involve the spinal cord or peripheral nervous system but not the brain; alternatively, pseudodystonia may be caused by non-neurological diseases, including arthritis and other musculoskeletal diseases [2,3]. We report a rare case of pseudodystonia caused by syringomyelia.
A 20-year-old woman presented to our clinic with a 2-month history of paroxysmal painful stiffness in all her limbs. Two months before this visit, she felt stiffness in her right arm. She could not flex her fingers, and she experienced a tingling sensation and severe pain throughout the limb. The stiffness disappeared 20 minutes later. Two days later, in the morning, she felt stiffness and weakness in the right arm and leg, which also disappeared 20 minutes later. Similar episodes occurred in the left limbs; in fact, they appeared two or three times a day, alternating between the left and right limbs. The patient had no past medical history or family history of such a disorder. Additionally, there was no history of trauma. She was hospitalized and underwent a detailed neurological examination and further evaluation.
The neurological examination revealed dystonic tremor in the outstretched position in the right arm, and the pin-prick sensation was impaired in the right limbs, but proprioception was preserved. Hemiparesis in the right limbs was scored 4+ according to the Medical Research Council scale for muscle power.
Upon admission, she exhibited a dystonic attack with a pattern of sustained twitching in a fixed posture regardless of rest or action for approximately 20 minutes, which alternated between the left and right limbs one to three times a day. The attack involved the elbows and the lower part in the arms. Sensory tricks were absent. Independently, dystonic tremor was observed in the outstretched position, which was more prevalent on the right side. Dystonic tremor of the right hand and dystonic attack in the left limbs were recorded on video (Supplementary Video 1 in the online-only Data Supplement).
Laboratory testing revealed no abnormalities in the complete blood cell count; electrolyte levels; renal, liver, or thyroid function; copper, ceruloplasmin, iron, ferritin, vitamin B12, folate, or C-reactive protein levels; total iron-binding capacity; erythrocyte sedimentation rate; or fibrinogen degradation production. Tests for D-dimer and a coagulation battery also showed normal ranges, as did serum and urine protein electrophoresis. Paraneoplastic antibody testing and Sanger sequencing for the TOR1A, SGCE, and GCH1 genes yielded negative results. Electroencephalogram revealed no epileptiform discharge.
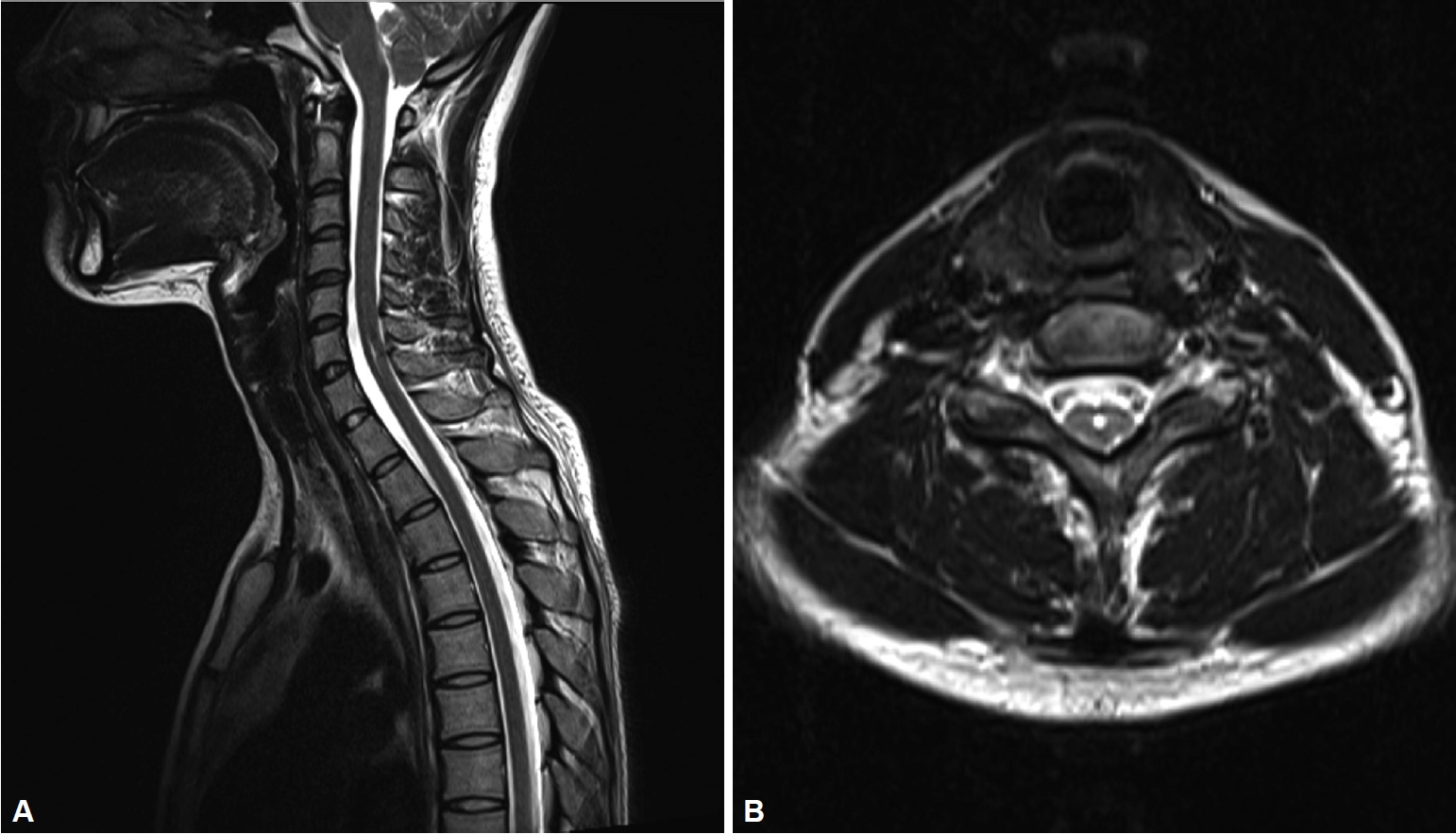
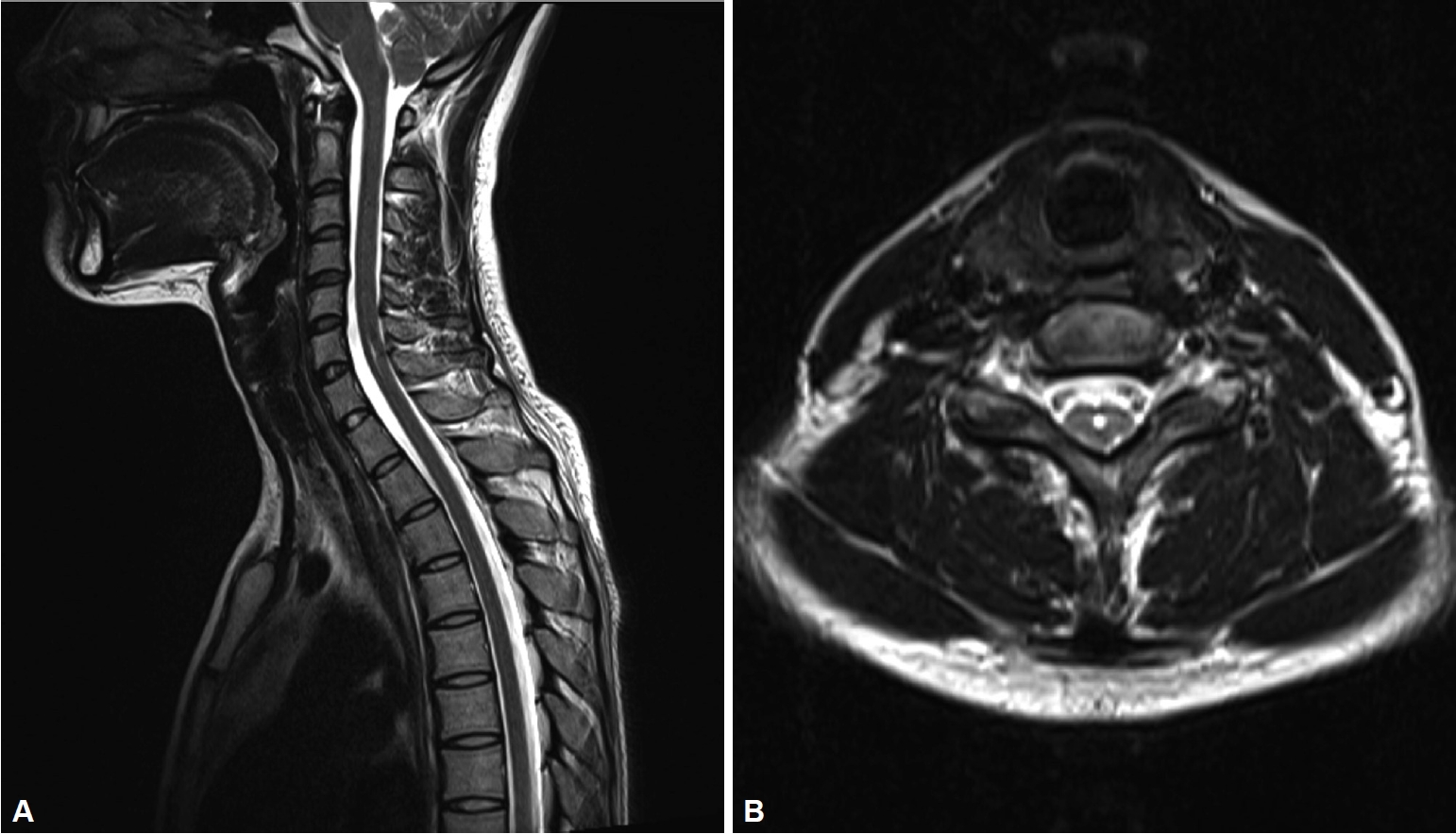
Cervical magnetic resonance imaging (MRI) revealed mild dilatation of the central canal along levels C2–C7, which was suggestive of a syrinx (Figure 1). Brain MRI findings were normal.
In motor evoked potential (MEP) testing, recorded in both abductor digiti quinti, amplitudes were significantly decreased, with delayed latencies after cortical stimulation. Amplitudes were decreased more on the left side than on the right but were within the normal range after cervical stimulation. Amplitudes were symmetrically normal after the stimulation of Erb’s point. MEPs recorded in both tibialis anterior regions were not obtainable after cortical stimulation but were normal after lumbar stimulation. These findings suggested conduction block in the corticospinal tract between the cortical and cervical spinal levels. The final diagnosis was pseudodystonia caused by syringomyelia. Levodopa, trihexyphenidyl, atenolol, and clonazepam were administered but had no effect, and the patient was lost to follow-up 3 months after the diagnosis.
This patient showed abnormal muscle contraction and posturing of the involved limb, which mimicked paroxysmal dystonia. The clinical features of coexistent motor and sensory abnormalities such as hemiparesis and impaired sensation, an absence of sensory tricks, acute onset and co-occurring severe pain suggested the diagnosis of pseudodystonia rather than true dystonia [3]. Fixed twitching in the left or right limbs occurred regardless of action or a resting state and had no overflow activity, and these findings were inconsistent with true dystonia [2].
Syringomyelia may manifest with abnormal movements, including dystonia, tremor, and athetosis [4]. Dystonia associated with syringomyelia was first reported in 1983, and 18 definite cases have been described since [4]. Syringomyelia usually manifests with bilateral sensory and motor symptoms, including pain, stiffness, and weakness in the extremities [5]. A loss of pain and temperature sensation (the maintenance of proprioception) are typical sensory symptoms of syringomyelia, and T2-weighted MRI, the imaging modality used to diagnose this condition, demonstrates hyperintense uptake in the syrinx [6]. MEP tests show the absence of motor responses in affected limbs [7].
The pathogenesis of dystonia-mimicking muscle contractions with syringomyelia remains uncertain, and descriptions of the pathogenesis of pseudodystonia caused by syringomyelia in the literature are limited [3,6]. Mulroy et al. [4] proposed several potential causes that included both motor and sensory mechanisms: abnormalities in sensorimotor integration and a loss of neural inhibition. Abnormal thresholds in spatial and temporal discrimination and abnormal gating of sensory information are found in patients with dystonia, which promote abnormal correction with abnormal motor actions that resemble dystonia. A loss of neural inhibition at the level of the spinal cord and in the brain also plays a role in the pathogenesis of dystonic movement, resulting in co-contraction of agonist and antagonist muscles [4]. In our patient, the lesion in the spinal cord may have caused the loss of neural inhibition. The mechanisms underlying the episodic paroxysmal pattern are unclear, but the possibility that local sensory input triggered this symptom was considered [4].
Effective treatment for pseudodystonia remains uncertain, and the long-term effects of the decompression of syringomyelia on pseudodystonia have not been reported in the literature to our knowledge. Unfortunately, our patient did not respond to the medications and did not undergo decompression surgery in our clinic. In addition, the cause of her syringomyelia was not found.
In conclusion, this case of pseudodystonia caused by syringomyelia illustrated typical clinical features of pseudodystonia that should be considered when irrelevant symptoms are accompanied by abnormal muscle contraction or posturing.
Dystonic tremor of the right arm is observed in an outstretched position. During a dystonic attack, the left upper limb shows stiffness and abnormal fixed posturing. The patient had gait disturbance because of stiffness and abnormal muscle contractions in the left leg.
Notes
Ethics Statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Declaration of Helsinki and its later amendments or comparable ethical standards. Written informed consent was obtained from the patient.
Conflicts of Interest
The authors have no financial conflicts of interest.
Funding
This study was supported by the Korea Healthcare Technology R&D Project, Ministry of Health & Welfare, Republic of Korea (grant number: HI19C0256).
Author Contributions
Conceptualization: Yun Su Hwang, Sungyang Jo. Data curation: Yun Su Hwang, Sungyang Jo. Formal analysis: Yun Su Hwang. Funding acquisition: Sun Ju Chung. Investigation: Yun Su Hwang. Methodology: Yun Su Hwang. Project administration: Yun Su Hwang. Resources: Yun Su Hwang, Seung Hyun Lee. Software: Yun Su Hwang, Seung Hyun Lee. Supervision: Sun Ju Chung. Validation: Sun Ju Chung. Visualization: Yun Su Hwang. Writing—original draft: Yun Su Hwang. Writing—review & editing: Sun Ju Chung.
Figure 1.
Magnetic resonance imaging of the cervical spine of the patient. A: T2-weighted sagittal image of the cervical spine shows the dilatation of the central canal along the levels of C2–C7, particularly at C5–C7. B: The axial view of levels of C5–C7 shows the dilatation of the central canal, which is suggestive of a syrinx.
REFERENCES
1. Kojovic M, Pareés I, Kassavetis P, Palomar FJ, Mir P, Teo JT, et al. Secondary and primary dystonia: pathophysiological differences. Brain 2013;136(Pt 7):2038–2049.ArticlePubMed
2. Albanese A, Bhatia K, Bressman SB, Delong MR, Fahn S, Fung VS, et al. Phenomenology and classification of dystonia: a consensus update. Mov Disord 2013;28:863–873.ArticlePubMedPMC
3. Berlot R, Bhatia KP, Kojović M. Pseudodystonia: a new perspective on an old phenomenon. Parkinsonism Relat Disord 2019;62:44–50.ArticlePubMed
4. Mulroy E, Balint B, Latorre A, Schreglmann S, Menozzi E, Bhatia KP. Syringomyelia-associated dystonia: case series, literature review, and novel insights. Mov Disord Clin Pract 2019;6:387–392.ArticlePubMedPMC
6. Sternberg ML, Gunter ML. Syringomyelia. J Emerg Med 2017;53:e31–e32.ArticlePubMed
7. Nardone R, Höller Y, Thomschewski A, Höller P, Bergmann J, Golaszewski S, et al. Central motor conduction studies in patients with spinal cord disorders: a review. Spinal Cord 2014;5:420–427.Article
 E-submission
E-submission
 , Seung Hyun Lee
, Seung Hyun Lee
 PubReader
PubReader ePub Link
ePub Link Cite
Cite