E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 14(1); 2021 > Article
-
Original Article
Impact of Upper Eyelid Surgery on Symptom Severity and Frequency in Benign Essential Blepharospasm -
Hannah Mary Timlin, Kailun Jiang
 , Daniel George Ezra
, Daniel George Ezra -
Journal of Movement Disorders 2021;14(1):53-59.
DOI: https://doi.org/10.14802/jmd.20075
Published online: January 12, 2021
Blepharospasm Clinic, Moorfields Eye Hospital NHS Foundation Trust, London, UK
- Corresponding author: Hannah Mary Timlin, BSc, FRCOphth, MBChB Adnexal Office, Moorfields Eye Hospital, 162 City Road, London EC1V2PD, UK / Tel: +44-20-7253-3411 / Fax: +44-20-7566-2334 / E-mail: hannahtimlin@nhs.net
Copyright © 2021 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objective
- To assess the impact of periocular surgery, other than orbicularis stripping, on the severity and frequency of blepharospasm symptoms.
-
Methods
- Consecutive patients with benign essential blepharospasm (BEB) who underwent eyelid/eyebrow surgery with the aim of improving symptoms were retrospectively reviewed over a 5-year period. Patients who had completed the Jankovic Rating Scale (JRS) and Blepharospasm Disability Index (BDI) pre- and at least 3 months postoperatively were included.
-
Results
- Twenty-four patients were included. JRS scores significantly improved from 7.0 preoperatively to 4.1 postoperatively (p < 0.001), and BDI scores significantly improved from 18.4 preoperatively to 12.7 postoperatively (p < 0.001); the mean percentage improvements were 41% and 30%, respectively. Patients were followed for a median of 24 months postoperatively.
-
Conclusion
- Periocular surgery significantly reduced BEB symptoms in the majority (83%) of patients by an average of 33% and may therefore be offered for suitable patients. An important minority (17%) of patients experienced symptom worsening.
- This study was approved by the Moorfields Eye Hospital NHS Trust Audit Committee (study number CA16/AD/20) and was conducted in accordance with the Declaration of Helsinki.
- Case inclusion criteria
- Consecutive patients with BEB who underwent eyelid/eyebrow surgery with the aim of reducing eyelid closure or spasm symptoms were retrospectively reviewed over a 5-year period between 2012 and 2016 from one consultant’s operating lists. Patients who had completed the Jankovic Rating Scale (JRS) [8] and Blepharospasm Disability Index (BDI) [9] preoperatively and at least three months postoperatively were included.
- Data analysis
- Data were analyzed using Prism 8.0.2 (GraphPad Software, Inc., San Diego, CA, USA). Preoperative and postoperative JRS and BDI scores were compared using the two-tailed Wilcoxon matchedpairs signed rank test. Statistical significance was taken at p < 0.05.
- Criteria for surgery
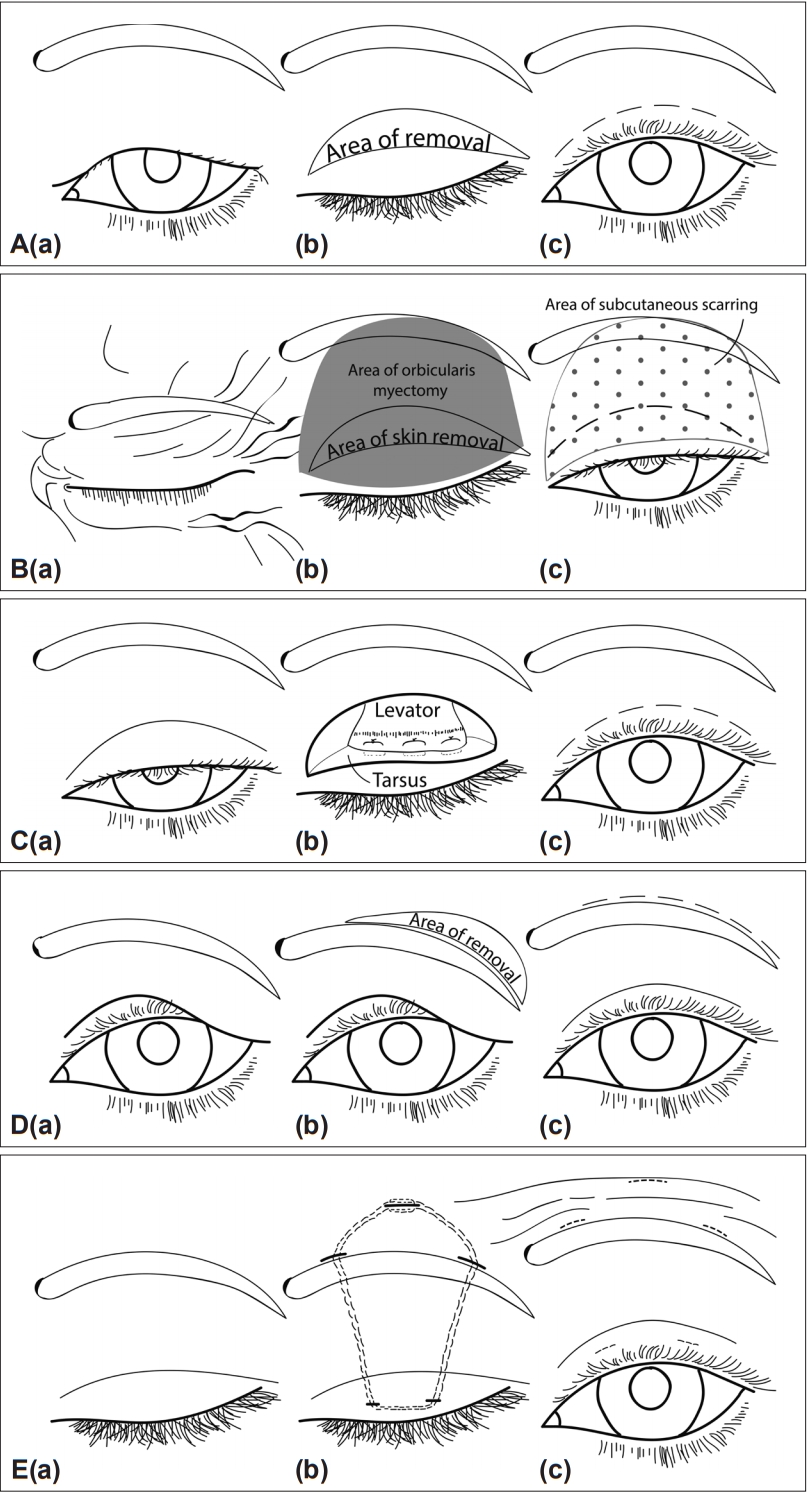
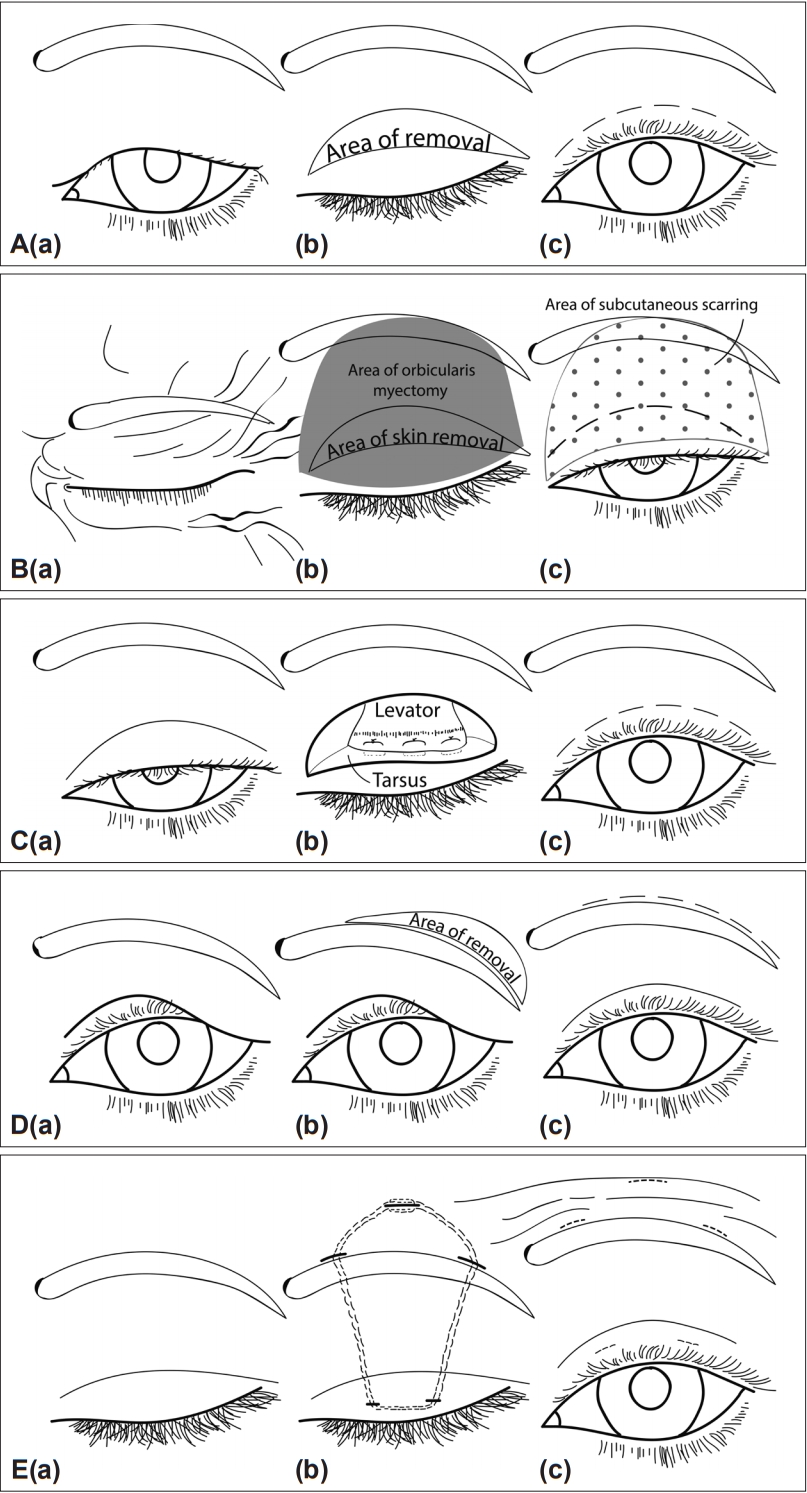
- BEB patients who had upper eyelid skin sitting on or hanging over the upper eyelid lashes (dermatochalasis) [Figure 1A(a)] with pretarsal orbicularis spasms were offered upper lid blepharoplasty. In upper lid blepharoplasty, an upper lid skin crease incision was made and extended laterally. Excess skin was pinched with the eyes closed and marked to ensure that enough skin remained to allow for complete eyelid closure. A crescent shape of skin was removed along with the underlying orbicularis muscle [Figure 1A(b)]. The skin edges were then sutured together [Figure 1A(c)]. This was in contrast to orbicularis stripping, where the orbicularis muscle was extensively undermined and removed in toto from the lashes to above the eyebrow (Figure 1B).
- BEB patients with upper eyelid ptosis as defined by a low-sitting lid margin (> 2 mm from the central cornea to the upper lid margin) [Figure 1C(a)] and pretarsal orbicularis spasms were offered ptosis repair. In ptosis surgery, a skin crease incision was made and extended down onto the tarsus. The levator aponeurosis was then isolated, plicated, shortened, and sutured back onto the tarsus [Figure 1C(b)]. The skin was closed, incorporating small fibres of the aponeurosis to reform the skin crease [Figure 1C(c)].
- BEB patients with brow ptosis (eyebrow sitting below the superior orbital rim) [Figure 1D(a)] and orbital orbicularis spasms were offered a direct brow lift. In a direct brown lift, a crescent shape of skin and subcutaneous fat were removed from above the lateral 3/4 of the brow [Figure 1D(b)]. The defect was closed with deep and subcuticular sutures [Figure 1D(c)].
- Eyelid opening apraxia was defined as a nonparalytic inability to open the eyes despite conscious effort [Figure 1E(a)] in the absence of visible orbicularis contraction [10]. Frontalis sling surgery was offered to these BEB patients with eyelid opening apraxia. A supramid nylon suture or silicon tube was used to couple the tarsus to the frontalis muscle of the forehead in a pentagon shape [Figure 1E(b)]. Through 2 pretarsal and 3 forehead stab incisions, the suture was passed through the anterior tarsus and was then passed superiorly in the sub-orbicularis plane to the brow and forehead. The suture was tied and buried in the forehead once the eyelid height and shape were satisfactory [Figure 1E(c)].
MATERIALS & METHODS
- Patient demographics
- Twenty-four patients with a median age of 62 years (range 46 to 80) met the inclusion criteria. Eighteen patients (75%) were female. They had been diagnosed with BEB for a mean of 8 years (range 2 months to 24 years). Additional diagnoses of Meige syndrome and eyelid opening apraxia were made in 4 (17%) and 9 (38%) patients, respectively.
- Previous BEB treatment
- All patients had regular BTIs, 23 (96%) were using lubricants, and 1 (4%) had previously tried punctal plugs. Six (25%) patients were on systemic medication for BEB at the time of surgery (2 were on trihexyphenidyl, and 4 were on sedative medication). Another 6 patients had previously tried and stopped trihexyphenidyl. A significant subset of patients were using spectacle aids: 4 (17%) were using the FL41 tint, 1 (4%) was using pressure pad mounted glasses, and 1 (4%) was using ptosis props. One (4%) patient had undergone previous intracranial electrode placement, and 5 (21%) had undergone previous eyelid/brow surgery.
- Periocular surgery
- Periocular surgeries included 16 blepharoplasties (80%) for the treatment of dermatochalasis, 8 ptosis repairs through levator advancement (45%), 8 direct brow lifts for brow ptosis (40%), and 7 frontalis slings for the treatment of eyelid opening apraxia (35%). Fourteen (58%) individuals underwent a combination of procedures (Table 1). No surgical complications were observed.
- Postoperative scores
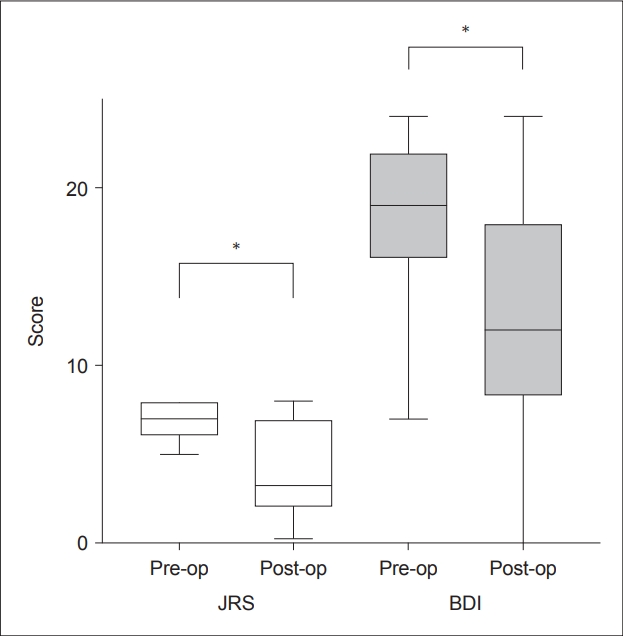
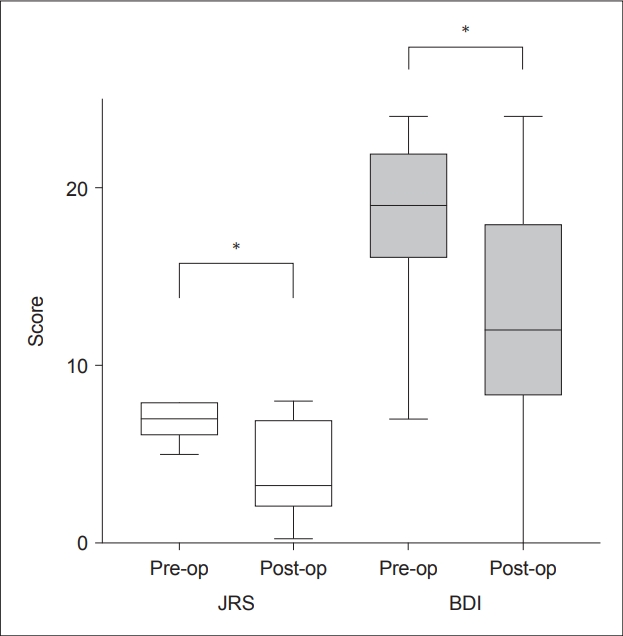
- The median time from surgery to postoperative scoring was 24 months (range 4 to 48 months). The time to their postoperative score from their last BTI was a median of 3 months (range 2 days to 35 months). The mean preoperative JRS score was 7.0, which improved to 4.1 postoperatively and was statistically significant (p < 0.001), with a mean improvement of 2.9 points (41%) (Figure 2). The mean preoperative BDI score was 18.4, which improved to 12.7 postoperatively and was statistically significant (p < 0.001), with a mean improvement of 5.7 points (30%) (Figure 2).
- When the JRS and BDI scores were combined (added), 20 (83%) patients showed improvement in their symptoms (lower postoperative score), whereas 4 (17%) had symptom worsening following surgery (higher postoperative score). Compared to their preoperative scores, patients’ combined symptom scores improved by a mean of 33% (range -56% to 98%). Scores were taken 11.6 weeks (mean) after the latest preoperative BTI compared to 17.4 weeks (mean) after the latest postoperative BTI, which was not significantly different (p = 0.23) (Table 1).
- Postoperative botulinum toxin
- The postoperative botulinum toxin dose was identified in 19 patients. The BTI units of Xeomin and Dysport were reduced from a mean of 100 iU preoperatively to 58 iU postoperatively, which was not significant (p = 0.1). BTIs were restarted in 1 patient with some effect, while there was no effect preoperatively. Three (16%) patients chose not to receive further BTIs following surgery: one because the spasms had stopped, another because the spasms were improved and the last because the BTIs only provided benefits for 2–4 weeks. The BTI dosing gaps were documented in 10 patients pre- and postoperatively. This increased from 11.6 to 12.7 weeks, which was not significantly different (p = 0.57) (Table 1).
RESULTS
- Orbicularis stripping has been the classic surgical option to reduce spasm severity in BEB patients, with reports of 50% of patients being free from troublesome spasms 30 months after surgery [11]. However, this surgery has decreased in popularity due to the availability and efficacy of BTIs [12]. Orbicularis stripping can result in poor cosmetic outcomes with adherent visibly scarred skin contracture [13], orbital septal scarring [14], chronic lymphoedema, and lagophthalmos [11]. Worse yet, these patients may experience severe pain during further injections of botulinum toxin into the scarred tissues. Thus, orbicularis stripping is now rarely performed in the authors’ department.
- This study suggested that non-orbicularis stripping periocular surgeries, such as blepharoplasty, ptosis surgery, direct brow lifts, and frontalis sling surgery, could reduce the severity of BEB symptoms when measured using the JRS and BSI scoring systems. Non-orbicularis stripping periocular surgeries on average reduced BEB symptoms by one-third. While not statistically significant, there was a trend towards a reduced BTI dose postoperatively and a longer time between symptom scoring and the previous BTI postoperatively. These serve as important internal controls indicating that the reduced symptom severity was not a result of the increased BTI dose or more recent BTI use. The results of this study reinforce the knowledge that lid surgery is not a complete cure but can provide symptom reduction in the majority of people. This information is vital for managing patient expectations when reviewing treatment options.
- Symptom scores were higher postoperatively in 4 (17%) patients. Although this could be a direct consequence of surgery, BEB is known to typically progress with time, resulting in increased symptom frequency, severity, and spread of muscle involvement [15-17]. Indeed, Swope [15] remarked that symptomatic treatments do not alter the natural history of BEB.
- Frontalis sling surgery has previously been shown to be effective in blepharospasm patients with eyelid opening apraxia, improving their quality of life assessed through a questionnaire and self-assessment calendar [18]. Interestingly, Dressler et al. [18] reported 27% complete symptom resolution following frontalis slings combined with regular postoperative BTIs. In our brow suspension cohort of patients, who similarly continued with BTIs, a reduction in the combined symptom score of 27% was achieved, albeit without complete remission.
- Although no side effects were documented for the patients reviewed in this study, in general, the main side effect of these eyelid procedures is dry eye symptom worsening due to increased palpebral aperture and reduced eyelid closure. Patients were counselled to increase lubricant drops during the day and ointment at night postoperatively.
- Beyond the inclusion period, the authors noted a postoperative complication worth mentioning. A patient underwent frontalis suspension for BEB with parkinsonism due to progressive supranuclear palsy. The sling eroded through the conjunctiva, leading to corneal thinning and descemetocele. The ocular surface was further compromised by lagophthalmos and incomplete blinking as a result of the sling. This complication is perhaps more common in patients with both Parkinson’s disease and BEB than in patients with BEB alone due to the reduced blink rate [19] and profound eyelid opening apraxia in Parkinson’s disease, especially progressive supranuclear palsy.
- Although patient examination findings vary, for ease of understanding, they can be summarized into three broad groups. First, patients presenting with a low upper eyelid position due to levator aponeurosis dehiscence may benefit from ptosis repair surgery. Ptosis is commonly observed in BEB patients and may be due to mechanical fatigue at the levator aponeurosis insertion as a result of excessive blinking. Ptosis results in even minor spasms obscuring the visual axis. Second, patients presenting with orbital orbicularis spasms may benefit from a direct brow lift and upper lid blepharoplasty. Similar mechanical stresses to soft tissue in the upper eyelid causing ptosis may be responsible for significant brow ptosis and dermatochalasis in BEB. A direct brow lift and upper lid blepharoplasty may reduce the blinking threshold by reducing the heaviness of the upper lids and/or skin hanging over the lashes. Finally, patients presenting with mainly eyelid opening apraxia may benefit from frontalis sling surgery, where the lifting of the upper lid is tethered to the action of the frontalis muscle and thereby bypasses the inhibited levator muscle in BEB. As the number of patients undergoing surgery increases, we hope to be able to analyze the three different groups of eyelid/eyebrow operations separately for more specific outcomes.
- Limitations
- Standardized scores were recorded as snapshots, which do not reflect the inherent fluctuation of symptom severity. In addition, the score timing did not coincide with the same point in the patient’s BTI cycle. As BEB is known to be a lifelong condition, longer follow-up would be useful for future studies to determine the impact over a longer course.
- Conclusion
- In summary, non-orbicularis stripping periocular surgery can significantly improve BEB symptoms in the majority (83%) of patients, with an average reduction in symptoms of 33%. It is therefore an important contribution towards improving these patients’ quality of life. A minority (17%) of patients experience worsening of symptoms despite surgery, and they should be warned of this during the surgical decision-making process.
DISCUSSION
-
Conflicts of Interest
Dr. Timlin and Dr. Jiang have no conflicts of interest. Dr. Ezra receives funding from the NIHR Biomedical Research Center for Ophthalmology at Moorfields Eye Hospital and University College London- Institute of Ophthalmology.
-
Ethical Standard
The authors confirm that the approval of an institutional review board and patient consent was not required for this work, as it was based on retrospective data previously collected for patient care. The Moorfields Eye Hospital NHS Trust Audit Committee authorized this decision and provided authorization, study number CA16/AD/20. This study was conducted in accordance with the Declaration of Helsinki. Informed consent was therefore not required to be obtained. We confirm that we have read the journal’s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.
-
Author Contributions
Conceptualization: Hannah Mary Timlin, Daniel George Ezra. Data curation: Hannah Mary Timlin, Kailun Jiang. Formal analysis: Hannah Mary Timlin, Kailun Jiang. Investigation: Hannah Mary Timlin. Methodology: Hannah Mary Timlin. Project administration: Hannah Mary Timlin. Resources: Hannah Mary Timlin, Kailun Jiang. Software: Hannah Mary Timlin, Kailun Jiang. Supervision: Daniel George Ezra. Validation: Hannah Mary Timlin, Kailun Jiang. Visualization: Hannah Mary Timlin, Kailun Jiang. Writing—original draft: Hannah Mary Timlin. Writing—review & editing: all authors.
Notes
- None.
Acknowledgments
- 1. Costa J, Espírito-Santo C, Borges A, Ferreira JJ, Coelho M, Moore P, et al. Botulinum toxin type A therapy for blepharospasm. Cochrane Database Syst Rev 2005;(1):CD004900.Article
- 2. Meige H. Les convulsions de la face: une forme clinique de convulsion faciale, bilaterale et mediane. Rev Neurol (Paris) 1910;21:437–443.
- 3. Kenney C, Jankovic J. Botulinum toxin in the treatment of blepharospasm and hemifacial spasm. J Neural Transm (Vienna) 2008;115:585–591.ArticlePubMed
- 4. Fayers T, Shaw SR, Hau SC, Ezra DG. Changes in corneal aesthesiometry and the sub-basal nerve plexus in benign essential blepharospasm. Br J Ophthalmol 2015;99:1509–1513.ArticlePubMed
- 5. Kilduff CL, Casswell EJ, Salam T, Hersh D, Ortiz-Perez S, Ezra D. Use of alleviating maneuvers for periocular facial dystonias. JAMA Ophthalmol 2016;134:1247–1252.ArticlePubMed
- 6. Lorenzano D, Tansley S, Ezra DG. Sensory trick frames: a new device for blepharospasm patients. J Mov Disord 2019;12:22–26.ArticlePubMedPMC
- 7. Georgescu D, Vagefi MR, McMullan TF, McCann JD, Anderson RL. Upper eyelid myectomy in blepharospasm with associated apraxia of lid opening. Am J Ophthalmol 2008;145:541–547.ArticlePubMed
- 8. Jankovic J, Orman J. Botulinum A toxin for cranial-cervical dystonia: a double-blind, placebo-controlled study. Neurology 1987;37:616–623.ArticlePubMed
- 9. Goertelmeyer S, Brinkmann G, Comes A, Delcker A. The Blepharospasm Disability Index (BSDI) for the assessment of functional health in focal dystonia. Clin Neurophysiol 2002;113(Suppl 1):S77–S78.
- 10. Boghen D. Apraxia of lid opening: a review. Neurology 1997;48:1491–1494.ArticlePubMed
- 11. Bates AK, Halliday BL, Bailey CS, Collin JR, Bird AC. Surgical management of essential blepharospasm. Br J Ophthalmol 1991;75:487–490.ArticlePubMedPMC
- 12. Arthurs B, Flanders M, Codère F, Gauthier S, Dresner S, Stone L. Treatment of blepharospasm with medication, surgery and type A botulinum toxin. Can J Ophthalmol 1987;22:24–28.PubMed
- 13. Clark J, Randolph J, Sokol JA, Moore NA, Lee HBH, Nunery WR. Surgical approach to limiting skin contracture following protractor myectomy for essential blepharospasm. Digit J Ophthalmol 2017;23:8–12.ArticlePubMed
- 14. Sagili S, Malhotra R. Skin contracture following upper eyelid orbiculectomy: is primary skin excision advisable? Orbit 2013;32:107–110.ArticlePubMed
- 15. Swope DM. Blepharospasm. In: Kompoliti K, Metman V, editors. Encyclopedia of Movement Disorders. 1st ed. Oxford: Academic Press; 2010:139–141.
- 16. Rucker JC. Normal and abnormal lid function. Handb Clin Neurol 2011;102:403–424.ArticlePubMed
- 17. Evatt ML, Freeman A, Factor S. Adult-onset dystonia. Handb Clin Neurol 2011;100:481–511.ArticlePubMed
- 18. Dressler D, Karapantzou C, Rohrbach S, Schneider S, Laskawi R. Frontalis suspension surgery to treat patients with blepharospasm and eyelid opening apraxia: long-term results. J Neural Transm (Vienna) 2017;124:253–257.ArticlePubMed
- 19. Fitzpatrick E, Hohl N, Silburn P, O’Gorman C, Broadley SA. Case-control study of blink rate in Parkinson’s disease under different conditions. J Neurol 2012;259:739–744.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
- The long-term response to botulinum toxin injections in patients with blepharospasm undergoing upper eyelid surgery
Assunta Trinchillo, Nunzia Cuomo, Francesco Habetswallner, Marcello Esposito
Parkinsonism & Related Disorders.2024; 119: 105958. CrossRef - Blepharospasm Secondary to Deep Brain Stimulation of the Subthalamic Nucleus in Parkinson Disease: Clinical Characteristics and Management Outcomes
Michelle A. Ting, Alexandra I. Manta, Emma Samia-Aly, Michelle Lai, Emanuel R. de Carvalho, Philip Buttery, Daniel G. Ezra
Journal of Neuro-Ophthalmology.2023;[Epub] CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite