Risk Factors for Falls in Patients with de novo Parkinson’s Disease: A Focus on Motor and Non-Motor Symptoms
Article information

Abstract
Objective
We aimed to identify risk factors for falls in patients with de novo Parkinson’s disease (PD).
Methods
Forty-six patients with de novo PD were retrospectively included in the study. We assessed details on the patients’ motor symptoms as well as non-motor symptoms using several representative scales for global cognition, depression, fatigue, and dysautonomia. Fallers and non-fallers were identified according to their history of falls during the preceding year.
Results
Twenty-two patients (45.8%) with de novo PD had a history of falls. Compared with the non-faller group, the faller group exhibited higher scores for postural instability/gait difficulty (PIGD), anxiety, fatigue, total dysautonomia, gastrointestinal dysfunction, and thermoregulatory dysfunction. Moreover, logistic regression analysis showed that falling was positively correlated with anxiety and gastrointestinal symptoms but negatively associated with the tremor scores.
Conclusion
Our findings suggest that falling in patients with de novo PD is significantly associated with PIGD/non-tremor symptoms, anxiety, and gastrointestinal dysfunction.
Falls are common and can decrease the quality of life of patients with Parkinson’s disease (PD). Accordingly, many researchers have studied methods of preventing or treating falls in PD patients. According to a review article, the proportion of patients with PD who have experienced at least one fall event was reported to be 35–90% (mean, 60.5%) [1]. Another review article revealed that the incidence of recurrent falls ranged from 18% to 65% (mean, 39%) in patients with PD [2]. Many factors, including an older age; severe motor symptoms; and gait/axial impairments, such as gait freezing, impaired cognition, a history of falls, a fear of falling, and a low health-related quality of life, have also been shown to be associated with falls in PD patients [3,4]. However, little is known about the risk factors for falls in individuals in the early stages of PD since the majority of studies on falls have been conducted in individuals in the relatively advanced stages of PD.
We were interested in the fall risk factors for patients with early stages of PD. Therefore, in this pilot study, we aimed to investigate motor and non-motor symptoms associated with falling in drug-naïve patients with de novo PD. Our findings may facilitate clinicians who treat patients with de novo PD identify groups at high risk for falls.
MATERIALS & METHODS
Participants
This study was approved by the Institutional Review Board of our institution (#2019-12-012). We carefully reviewed all the medical charts of patients first evaluated for parkinsonism in our movement disorder clinics between July 2017 and October 2019 and identified eligible patients with de novo PD according to the UK Brain Bank criteria [5]. Only patients who underwent both brain MRI and dopamine transporter imaging (DAT) were initially evaluated, and those with other parkinsonian disorders were excluded. Accordingly, strict inclusion and exclusion criteria were applied since this study was retrospectively designed. Patients showing not only typical striatal dopamine depletion with a rostrocaudal gradient in the putamen, as identified by DAT [6], but also typical clinical characteristics of PD and presenting with levodopa-responsive asymmetric parkinsonism were included. Patients exhibiting atypical findings, including putaminal abnormalities, cerebellar atrophy, middle cerebellar hyperintensity, the hot cross bun sign, hydrocephalus, or stroke-related lesions in the MRI findings, were excluded. Moreover, patients with atypical clinical features, including poor levodopa responsiveness, frequent falls, supranuclear gaze palsy, orthostatic hypotension, urinary incontinence, or significant cognitive impairment, were excluded. Out of a total of 56 patients, eight were excluded after the screening step. Two patients had normal pressure hydrocephalus, three had multiple system atrophy, one had progressive supranuclear palsy, one had drug-induced parkinsonism, and one had senile parkinsonism. Finally, 48 patients with de novo PD were included in the study.
Clinical assessments
When each patient was initially admitted to our movement disorder clinic, his or her history of falls within the last year was recorded. A meta-analysis revealed that previous falls over a period of 12 months were recorded in the majority (50%) of studies in PD patients [4], although the length of the period varied across studies (i.e., 3, 6, and 12 mo). A fall event was defined as when a person unexpectedly lost his or her balance and inadvertently rested on the ground, floor, or other low surface. We recorded the number of falls that each patient experienced during the preceding year. If a patient with PD answered ‘no,’ the patient was categorized as a non-faller. If any patient with PD reported experiencing one or more falls, then the patient was categorized as a faller for this study [7]. The baseline demographics and clinical characteristics, including motor and non-motor symptoms, were assessed. The total motor score was defined as the sum of the part III scores for the Unified Parkinson’s Disease Rating Scale (UPDRS). In addition, we calculated the subscores for tremor (the sum of the scores for UPDRS part III, items 3–9), rigidity (the sum of the scores for UPDRS part III, items 10–14), bradykinesia (the sum of the scores for UPDRS part III, items 15–22 and 27), and postural instability/gait difficulty (PIGD; the sum of the scores for UPDRS part II, items 13– 15 and UPDRS part III items 25 and 26) [8-10]. In addition, the Hoehn and Yahr (HY) stages were also assessed. Non-motor symptoms were evaluated by the Korean version of the Montreal Cognitive Assessment (MoCA-K) [11], the Korean version of the Beck Depression Inventory (BDI) [12], the Korean version of the Beck Anxiety Inventory (BAI) [13], the Parkinson’s Disease Fatigue Scale (PFS) [14], and the Korean version of the Scale for Outcomes in Parkinson’s Disease- Autonomic Dysfunction (SCOPA-AUT) [15].
Statistical analysis
The fallers and non-fallers with de novo PD were compared using Student’s t-test for the numerical data and the chi-squared test for the categorical data. Univariable logistic regression analyses were used for the binary outcomes, and a subsequent multivariable logistic regression analysis was performed by backward stepwise selection. A p-value of < 0.05 was considered statistically significant. All statistical analyses in the study were performed using SPSS (version 20.0, IBM Corp., Armonk, NY, USA).
Ethical standards
All procedures in the studies involving human participants were performed in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Helsinki declaration and its later amendments or comparable ethical standards. The need to obtain informed consent was waived by the IRB of our institution since this study is a retrospective study.
RESULTS
Comparison of clinical features between fallers and non-fallers with de novo PD
A total of 26 non-fallers and 22 fallers with de novo PD, who were grouped according to their histories of falls, were included in the study. The demographic and clinical characteristics, including motor and non-motor symptoms, between fallers and non-fallers with de novo PD are displayed in Table 1. Compared to the non-fallers with de novo PD, the fallers with de novo PD showed higher scores for PIGD (p = 0.040), anxiety (p = 0.029), fatigue (p = 0.019), and total dysautonomia (p = 0.024), as well as gastrointestinal and thermoregulatory subscores for dysautonomia (p = 0.020 and p = 0.047, respectively).
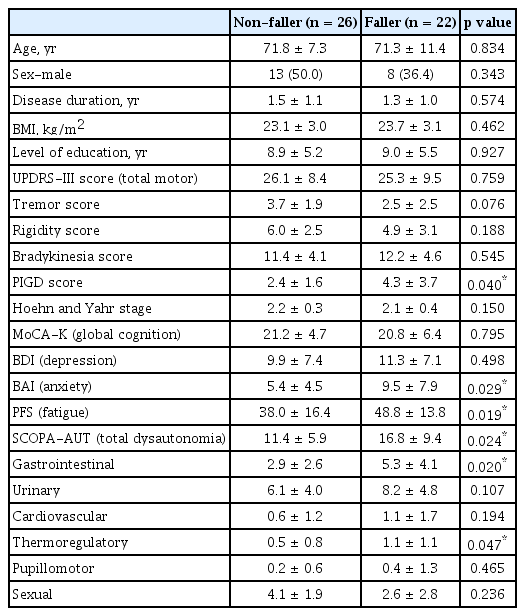
Demographics and clinical characteristics of de novo parkinsonian patients with and without falls
Risk factors for falls in patients with de novo PD
To identify the risk factors for falls in patients with de novo PD, we performed univariable and multivariable logistic regression analyses, as presented in Table 2. In the right column in Table 2, adjusted odds ratios (adj ORs) and 95% confidential intervals (95% CIs) are shown for the variables with significant results. We found that lower tremor scores were associated with the non-falling group of de novo PD patients (adj OR = 0.656, 95% CI = 0.459–0.938), whereas higher scores for anxiety and gastrointestinal symptoms correlated with the falling group of de novo PD patients (adj OR = 1.286, 95% CI = 1.020–1.300; adj OR = 1.286, 95% CI = 1.026–1.613, respectively).
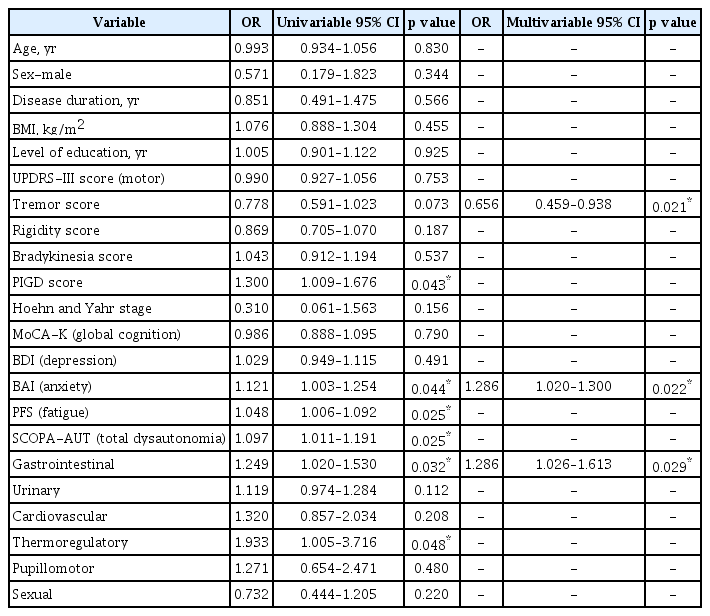
Logistic regression analysis of falls in patients with de novo Parkinson’s diseases
DISCUSSION
In this study, we found a high rate of falls (48.5%) during the preceding year in patients with de novo PD. Previously, a few studies have reported that 23% to 42% of patients with early PD experienced falls [3,16]. Moreover, a meta-analysis also revealed that fall frequency followed an inverted U-shaped curve in PD patients [4]. Collectively, our results suggest that patients with very early stages of PD may commonly experience falls. Therefore, clinicians need to be concerned for not only patients with advanced stages of PD but also patients with early stages of PD.
We evaluated the differences in the clinical characteristics between the falling and non-falling groups of drug-naïve patients with de novo PD. For the motor symptoms, the fallers with de novo PD showed higher PIGD scores than did the non-fallers with de novo PD (Table 1), whereas lower tremor scores were negatively associated with falling in patients with de novo PD (Table 2). Consistent with our results, Pelicioni et al. [17] showed that the PIGD subtype was related to falls compared to the non-PIGD subtype in PD patients. These findings suggest that patients with non-tremor-dominant PD might be at risk for falls. However, several non-motor symptoms, including anxiety, fatigue, total dysautonomia, gastrointestinal dysfunction, and thermoregulatory dysfunction, were associated with falls in patients with de novo PD (Table 1). Intriguingly, the logistic regression analyses revealed that only anxiety and gastrointestinal dysfunction were significantly related to falls in patients with de novo PD (Table 2). To the best of our knowledge, this is the first report showing a relation between both anxiety and gastrointestinal dysfunction and falling in PD patients. However, the pathomechanisms of how anxiety or constipation might be associated with falls in patients with de novo PD remain unknown. Moreover, our results should be interpreted with caution since this study has a relatively small sample size. Accordingly, more well-designed studies with larger sample sizes need to be conducted to address this issue.
In summary, the present study showed that falling is related to PIGD/less tremors, anxiety, and gastrointestinal dysfunction in patients with de novo PD. Clinicians need to pay attention to patients at a high risk for falls in the very early stages of PD.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Kyum-Yil Kwon. Data curation: Hyunjin Ju, Mina Lee, and Kayeong Im. Data analysis: all authors. Funding acquisition: KyumYil Kwon. Investigation: all authors. Methodology: Hyunjin Ju, Mina Lee, and Kayeong Im. Project administration: Kyum-Yil Kwon. Resources: Kyum-Yil Kwon. Supervision: Kyum-Yil Kwon. Validation: Kyum-Yil Kwon. Data visualization: all authors. Writing—original draft: Kyum-Yil Kwon. Writing—review & editing: all authors.
Acknowledgements
This work was supported by the Soonchunhyang University Research Fund and the National Research Foundation (NRF) of Republic of Korea (No. NRF2018R1C1B5045312).