This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
External ventricular drainage (EVD) is a lifesaving procedure for cerebrospinal fluid drainage in conditions such as tumor, trauma, hemorrhage, and hydrocephalus and is also used for intracranial pressure monitoring in intensive care units [1-4]. The freehand technique is a blind procedure that is often used in an emergency setting due to its simplicity and efficacy. It carries a risk of catheter malposition (6–36%), which can lead to brain injury, infection and hemorrhage [1,3]. The parenchymal injury is usually asymptomatic [3]. We report the first subject with acute hemichorea hemiballismus due to EVD malposition and discuss its management.
A 48-year-old male patient with no premorbid illness presented with acute onset generalized headache, recurrent episodes of vomiting and progressively decreasing sensorium over one day. He underwent emergency EVD insertion at an outside hospital and experienced severe abnormal movement in the right half of the body over the next 24 hours. He was on intravenous sedation and was referred to our center for further management. On examination, he was drowsy, and his cranial nerve examination was normal. His motor examination showed hypotonia with normal power in the right upper and lower limbs. There was hyporeflexia, and Babinski’s sign was positive on the right side. Muscle tone, power and reflexes on the left side were normal. He had irregular, involuntary, continuous choreiform movements in the distal right extremities with a proximal violent flinging component suggestive of hemichorea hemiballismus.
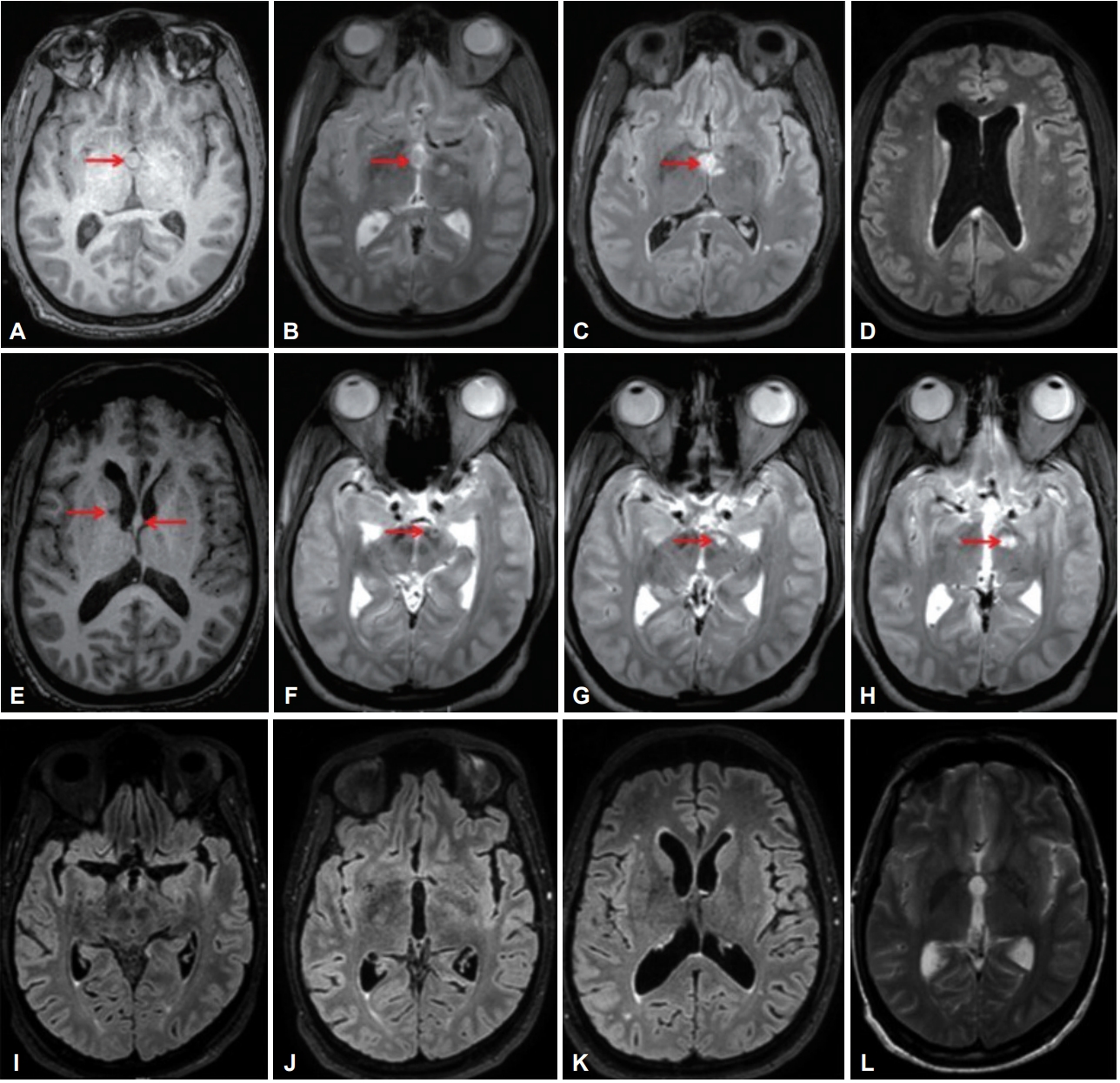
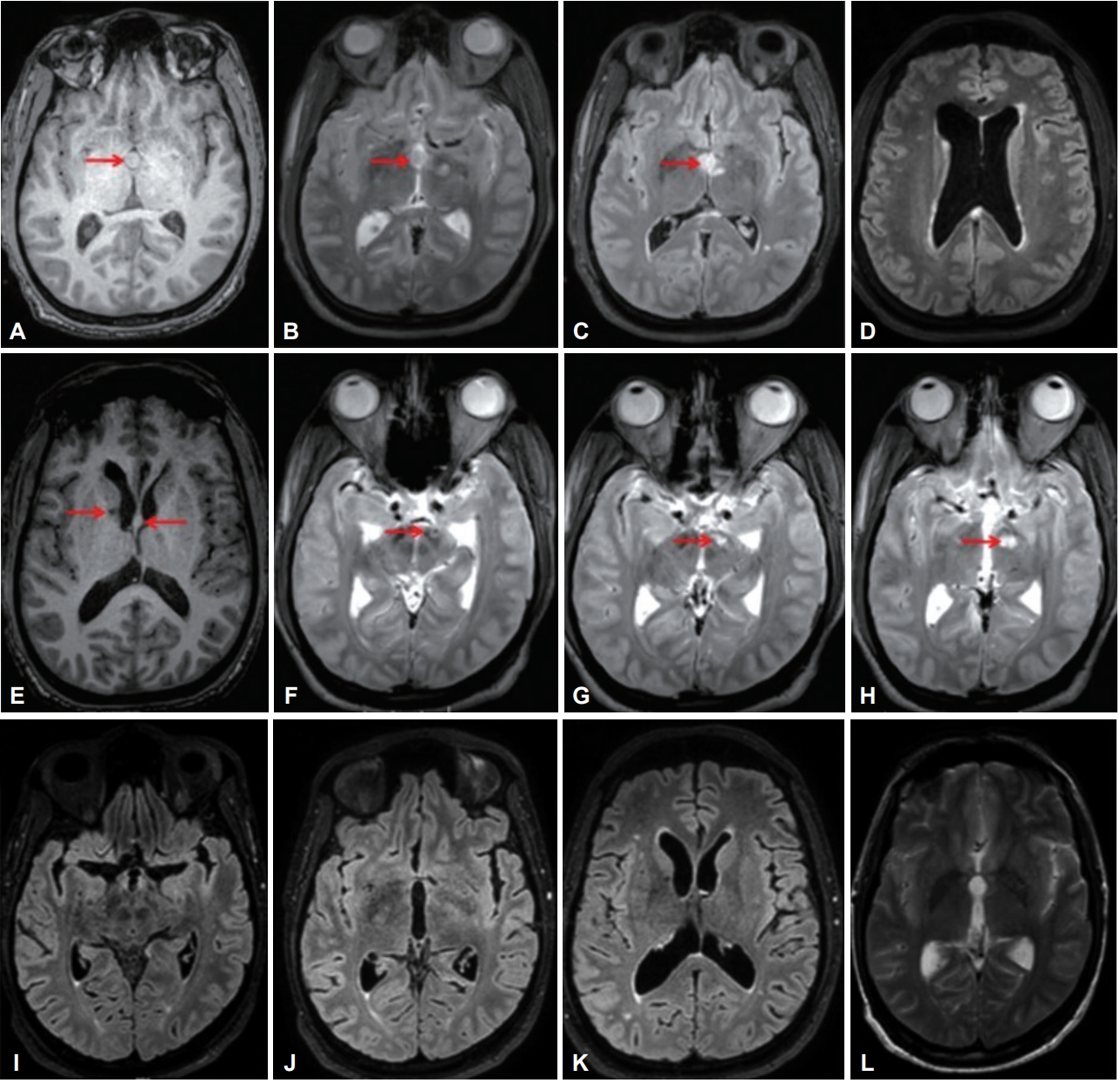
His blood sugar and electrolytes levels, hemogram, renal and liver profiles were normal. Brain MRI showed a well-defined lesion in the third ventricle, which was isointense on T1, hypointense on T2-weighted sequence and hyperintense on fluid-attenuated inversion recovery (FLAIR), suggesting a colloid cyst. The cyst produced foramen of Monro obstruction, leading to hydrocephalus (Figure 1). Imaging also showed parenchymal lesions in the right caudate, left substantia nigra, subthalamic nucleus (STN), globus pallidus and thalamus. These lesions were hypointense on T1 and hyperintense on T2-weighted sequence and showed diffusion restriction. The EVD tract was noted in the left STN (Figure 1). His cerebral angiogram was normal. He underwent lesion excision under general anesthesia, and the EVD was removed. The histopathology of the lesion was consistent with a colloid cyst.
The severe right hemichorea hemiballismus persisted during the postoperative period (Supplementary Video 1 in the online-only Data Supplement). He was managed with dexmedetomidine for two weeks, which was replaced by clonidine (0.15 mg/day) and morphine (30 mg/day). He also received intravenous haloperidol (15 mg/day) and oral tetrabenazine (150 mg/day) for his hyperkinetic movements. Haloperidol was replaced with oral risperidone (12 mg/day) after two weeks due to persistent symptoms. The risperidone dose was reduced to 3 mg/day after one week due to drug-induced leukopenia (total count: 1,600 cells/mm3, which improved to 8,300 cells/mm3 three days after the dose decrease). There was a mild decline in his right upper limb chorea at the end of one month (Supplementary Video 1 in the online-only Data Supplement). He was discharged on risperidone (3 mg/day), tetrabenazine (75 mg/day) and clonazepam (1 mg/day). There was gradual resolution of his movements, and he was symptom-free at the end of three months (Supplementary Video 1 in the online-only Data Supplement). His repeat MRI brain three months later was normal (Figure 1).
In summary, the patient had clinical features of acute obstructive hydrocephalus resulting from colloid cysts managed by EVD. The EVD malposition resulted in direct neuronal injury with hemichorea hemiballismus, as suggested by the lesions along the EVD tract. A vascular etiology was less likely because the lesions were in different vascular territories and his cerebral angiogram was normal. In head injury patients, STN lesions can produce hemichorea hemiballismus. These movements are usually persistent and show variable responses to medical and surgical therapy [5].
Colloid cysts are rare benign congenital intracranial lesions (0.2–2%) commonly seen in the third ventricular region (55% of third ventricular masses). Their clinical features include episodic headache, nausea and vomiting. Memory problems, behavioral changes, visual blurring, gait disturbances, and bowel and bladder incontinence are less frequent. A colloid cyst can also be an incidental imaging finding. A third ventricular cyst can obstruct the foramen of Monro, producing acute hydrocephalus, as observed in our patient [6]. Colloid cysts are hyperdense on brain CT. Their MRI findings are variable and depend on the cyst content. A cyst with high cholesterol content will reduce the T1-relaxation time, making it appear hyperintense on T1- weighted and hypointense on T2-weighted MRI sequences. In half of affected cases, T1 iso- or hypointensity is observed. Imaging can also reveal enlarged temporal horns or periventricular signal changes due to increased intraventricular pressure [6].
The ideal location of EVD is the ipsilateral frontal horn just anterior to the foramen of Monro. This is achieved in approximately 56% of patients via the freehand technique [1]. In EVD malposition, the catheter is located outside the ventricular system, requiring a second procedure for replacement [2]. The usual extraventricular sites were the Sylvian fissure, suprasellar cistern, interpeduncular cistern, frontal lobe, corpus collosum and basal ganglia [1,3]. The literature on catheter location and the clinical consequences of malposition is sparse [3]. Two studies reported basal ganglia, as common site of EVD malposition and no neurological sequale were observed [3,4].
The present case report adds iatrogenic injury to the exhaustive list of acquired chorea. In contrast to posttraumatic subjects, our patient achieved a good recovery with conservative treatment. These findings also highlight the risk of using the freehand technique for EVD insertion and necessitate an evaluation of image-guided methods to minimize the risk of neurological complications.
Video 1. Postoperative period: The patient had severe right hemichoreahemiballismus requiring intravenous sedation and ventilation support. Four weeks: He was conscious and oriented, and right hemichorea hemiballismus was observed. Twelve weeks: There was resolution of his choreiform movements. Written informed consent was obtained from the patient to publish his video.
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Figure 1.
MRI Brain. A-C: Colloid cyst on T1- and T2-weighted images and fluid-attenuated inversion recovery (FLAIR) sequence. Red arrows in A-C shows colloid cyst in T1,T2 and FLAIR image. D: FLAIR sequence showing a prominent lateral ventricle with periventricular lucencies suggestive of hydrocephalus. E: T1 sequence showing the external ventricular drainage (EVD) tract in the right caudate (right arrow), left globus pallidus and a colloid cyst in the septum pellucidum (left arrow). F: T2 sequence showing EVD tract located in the left subthalamic nucleus (red arrow). G and H: T2 hyperintensities in the left substantia nigra and left thalamus (red arrows). I-L: Brain MRI performed three months later showing resolution of the lesions on FLAIR (I-K) and T2 (L) sequences.
REFERENCES
1. Huyette DR, Turnbow BJ, Kaufman C, Vaslow DF, Whiting BB, Oh MY. Accuracy of the freehand pass technique for ventriculostomy catheter placement: retrospective assessment using computed tomography scans. J Neurosurg 2008;108:88–91.ArticlePubMed
2. Anderson RC, Kan P, Klimo P, Brockmeyer DL, Walker ML, Kestle JR. Complications of intracranial pressure monitoring in children with head trauma. J Neurosurg 2004;101(1 Suppl):53–58.ArticlePubMed
3. Hsieh CT, Chen GJ, Ma HI, Chang CF, Cheng CM, Su YH, et al. The misplacement of external ventricular drain by freehand method in emergent neurosurgery. Acta Neurol Belg 2011;111:22–28.PubMed
4. Saladino A, White JB, Wijdicks EF, Lanzino G. Malplacement of ventricular catheters by neurosurgeons: a single institution experience. Neurocrit Care 2009;10:248–252.ArticlePubMedPDF
5. Krauss JK, Jankovic J. Head injury and posttraumatic movement disorders. Neurosurgery 2002;50:927–939.ArticlePubMed
6. Algin O, Ozmen E, Arslan H. Radiologic manifestations of colloid cysts: a pictorial essay. Can Assoc Radiol J 2013;64:56–60.ArticlePubMed
Figure & Data
References
Citations
Citations to this article as recorded by
Efficacy and safety profile of neuroendoscopic hematoma evacuation combined with intraventricular lavage in severe intraventricular hemorrhage patients Hai‐Tao Ding, Yao Han, De‐Ke Sun, Quan‐Min Nie Brain and Behavior.2020;[Epub] CrossRef
 E-submission
E-submission
 , Ravi Gopal Varma, Nirmala Sankar, Raghavendra Pai
, Ravi Gopal Varma, Nirmala Sankar, Raghavendra Pai 

 PubReader
PubReader ePub Link
ePub Link Cite
Cite