This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
A 61-year-old male patient with a history of diabetes mellitus, hypertension and Hodgkin’s lymphoma (in remission over the last 20 years) was admitted due to visual disturbances and gait impairment which began abruptly 6 hours ago. On neurological examination, the patient was oriented and cooperated. Motor, sensory and cerebellar examinations were normal. However, a left-sided partial visual-field defect was apparent. In addition, gait difficulty (compatible with gait dyspraxia) was identified while he was walking. Cranial MRI showed diffusion restriction in the right occipital lobe (Figure 1). Laboratory investigations were unremarkable (hemogram, biochemistry, low-density lipoprotein: 67 mg/dL). Further investigations including brain/neck tomography angiography, echocardiography and 24-hourrhythm Holter were normal. With the diagnosis of cryptogenic stroke, the patient was discharged on aspirin therapy. On the sixth month of follow up at the polyclinic visit, the patient still suffered from gait difficulty and balance problems. He had experienced falling backwards several times since discharge. On neurological examination, a broad-based, cautious walking pattern was observed (Supplementary Video 1 in the online-only Data Supplement). In addition, postural instability was apparent such that the patient scored a 2 (would fall if not caught) on the Nutt retropulsion test (Supplementary Video 2 in the online-only Data Supplement) [1]. Confrontation visual field testing showed a bilateral normal visual field. Of note, for the investigation of visuoconstructive function, a clock drawing test was performed, which was normal. In addition, the Wechsler memory index (WMI)-IV (Visual Reproduction I subitem) was also performed, which was evaluated at 5/14 points (within the normal range, when normalized for age and education). He was referred to physical therapy for an intensive physical therapy program of proprioceptive and balance exercises.
Gait dyspraxia can be defined as a type of gait abnormality that cannot be explained by a demonstrable deficit in pyramidal, extrapyramidal, sensory, or cerebellar systems [2]. Gait dyspraxia is generally used to define the abnormal gait that accompanies cerebral small vessel disease, normal pressure hydrocephalus and some frontal lobe disorders. Based on the affected neuroanatomical regions and responsible pathophysiological mechanisms, Nutt [3] recently suggested a classification of two subtypes: anterior and posterior higher-level gait disorders (HLGD). We think that this index case represents a smart presentation of a patient with posterior HLGD. However, the reporting of cases with isolated gait dyspraxia following acute stroke (as in our case) is extremely rare in the literature [4]. Furthermore, the lesion site in the cuneus in our case was considerably localized providing substantial perspective on the clear role of this anatomical localization in locomotion. The cuneus is generally known for its involvement in basic visual processing. Considering that locomotion is a task that unarguably requires visuospatial processing, the mechanisms relating the outcome to the injury localization can be understood. On the other hand, the clock drawing test and WMIIV-Visual Reproduction I tests were in the normal ranges, which does not support the abovementioned hypothesis. However, we think that these cognitive tests might have failed to detect a mild deterioration in visuospatial function because they are not highly sensitive tests. Of note, and in accordance with this thought, the patient and his relatives had stated that he had significant difficulty performing these tests in his premorbid state. In the literature, the posterior parietal cortex and visuospatial attention have been repeatedly emphasized as critical for the execution of locomotion [5]. However, in a recent report using EEG/MEG methods, in addition to the frontal eye field and lateral intraparietal area, the cuneus was also identified as a critical region, involved in covert targeting of the task relevant stimulus marker (a process used in visual search) [6]. In accordance with that finding, several functional MRI studies have noted that the cuneus is a crucial localization and involved in shifting visual spatial attention [7]. Therefore, we still think that the ischemic injury in our patient might have disturbed the physiology of locomotion through a mechanism of malfunctioning visual spatial attention (which was beyond the scope of our cognitive tests).
Remarkably, it is known that gait dyspraxia can be present in marked disequilibrium with subsequent gait disturbance, without gait initiation failure, or without magnetic gait, as in this case [8]. Postural instability was a prominent finding in our patient. Postural stability is an essential component of locomotion, and maintaining postural stability requires multifactorial functions, including visual, somatosensory and vestibular sensations, in addition to muscle power. Neuroanatomically, a wide range of cortical areas and functional networks are known to be involved in the maintenance of postural stability. In a crucial report by Herb et al. [9], cerebral atrophy patterns associated with postural instability were specifically investigated in patients with Parkinson’s disease (PD). In that study, in addition to the atrophy of the bilateral frontal-temporal lobe, the cuneus was also demonstrated to be atrophic in these patients with postural instability. Therefore, the unique presentation of our patient with prominent postural instability, may also provide substantial perspectives regarding the physiology of postural stability.
However, an interesting question may be why the presentation of isolated gait dyspraxia (with postural instability) due to occipital lobe infarct is so rare in the literature [4], while stroke of the occipital lobe is a frequently encountered subtype in clinical practice. In an interesting study, patients with vestibular migraine, in whom the vestibular sensations were disrupted, were shown to have a higher visual dependency and lower stability of the postural control system [10]. Similarly, Konczak et al. [11] found that patients with PD showed better locomotor performances in visual cued locomotor tasks. In their conclusion, they hypothesized that the parietal cortex and related visuomotor functions, which are preserved in PD patients, compensated for the malfunctioning proprioceptive sensations (which have been shown to be disturbed in PD patients) during the execution of locomotion. Taken together, we hypothesize that the contribution of these systems to postural instability and locomotion may differ between individuals which may explain why this clinical outcome (gait dyspraxia) is observed in only some patients, but not in others. Nevertheless, in our patient, no comorbid diseases or features that could potentially disrupt somatosensory or vestibular sensations were present. Future reports with a larger number of these rare cases are surely warranted to clarify these discussions and add new perspectives to our understanding of the physiology of locomotion as well as the pathophysiology of higher-level gait disorders.
Broad-based and cautious gait and difficulty in turning.
Supplementary Video Legends
Video 2.
Significant postural instability (score of 2 on the Nutt retropulsion test).
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
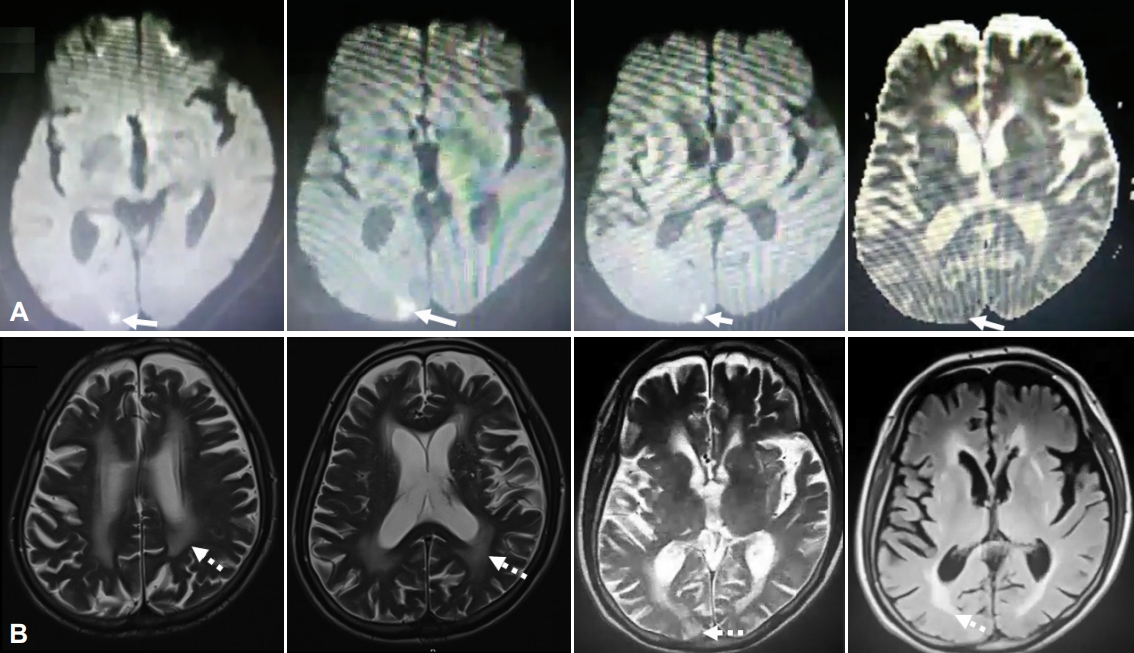
Figure 1.
A: Diffusion-weighted imaging sequences (the first three image) and apparent diffusion coefficient sequence (the last image) showing diffusion restriction in the right medial occipital lobe (particularly in the cuneus) (arrows). B: T2-weighted images showing diffuse white matter lesions (scattered arrows).
REFERENCES
1. Nutt JG, Marsden CD, Thompson PD. Human walking and higher-level gait disorders, particularly in the elderly. Neurology 1993;43:268–279.ArticlePubMed
2. Liston R, Mickelborough J, Bene J, Tallis R. A new classification of higher level gait disorders in patients with cerebral multi-infarct states. Age Ageing 2003;32:252–258.ArticlePubMedPDF
3. Nutt JG. Higher-level gait disorders: an open frontier. Mov Disord 2013;28:1560–1565.ArticlePubMed
4. Onder H. Dyspraxic gait due to right posterior cerebral artery stroke. J Neurosci Rural Pract 2018;9:162–164.ArticlePubMedPMCPDF
5. Menant JC, Sturnieks DL, Brodie MA, Smith ST, Lord SR. Visuospatial tasks affect locomotor control more than nonspatial tasks in older people. PLoS One 2014;9:e109802. ArticlePubMedPMC
6. Simpson GV, Weber DL, Dale CL, Pantazis D, Bressler SL, Leahy RM, et al. Dynamic activation of frontal, parietal, and sensory regions underlying anticipatory visual spatial attention. J Neurosci 2011;31:13880–13889.ArticlePubMedPMC
7. Asplund CL, Todd JJ, Snyder AP, Marois R. A central role for the lateral prefrontal cortex in goal-directed and stimulus-driven attention. Nat Neurosci 2010;13:507–512.ArticlePubMedPMCPDF
8. Briggs R, O’Neill D. Vascular gait dyspraxia. Clin Med (Lond) 2014;14:200–202.ArticlePubMedPMC
9. Herb JN, Rane S, Isaacs DA, Van Wouwe N, Roman OC, Landman BA, et al. Cortical implications of advancing age and disease duration in Parkinson’s disease patients with postural instability and gait dysfunction. J Parkinsons Dis 2016;6:441–451.ArticlePubMedPMC
10. Lim YH, Kim JS, Lee HW, Kim SH. Postural instability induced by visual motion stimuli in patients with vestibular migraine. Front Neurol 2018;9:433.ArticlePubMedPMC
11. Konczak J, Corcos DM, Horak F, Poizner H, Shapiro M, Tuite P, et al. Proprioception and motor control in Parkinson’s disease. J Mot Behav 2009;41:543–552.ArticlePubMed
Figure & Data
References
Citations
Citations to this article as recorded by
Relationship of Neural Correlates of Gait Characteristics and Cognitive Dysfunction in Patients with Mild Cognitive Impairment Yeo Jin Kim, Ingyu Park, Hui-Chul Choi, Moo-Eob Ahn, Ohk-Hyun Ryu, Daehun Jang, Unjoo Lee, Sang-Kyu Lee Journal of Clinical Medicine.2023; 12(16): 5347. CrossRef
 E-submission
E-submission
 , Ferda Buyuk2
, Ferda Buyuk2 

 PubReader
PubReader ePub Link
ePub Link Cite
Cite
