E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 12(1); 2019 > Article
-
Original Article
Sensory Trick Frames: A New Device for Blepharospasm Patients -
Daniele Lorenzano1
 , Steven Tansley2, Daniel G. Ezra1,3
, Steven Tansley2, Daniel G. Ezra1,3 -
Journal of Movement Disorders 2019;12(1):22-26.
DOI: https://doi.org/10.14802/jmd.18010
Published online: January 16, 2019
1Adnexal Service, Moorfields Eye Hospital, London, UK
2Spectacle Dispensing Department, Moorfields Eye Hospital, London, UK
3NIHR Biomedical Research Center for Ophthalmology, London, UK
- Corresponding author: Daniele Lorenzano, MD, https://orcid.org/0000-0001-8823-305X Adnexal Service, Moorfields Eye Hospital, 162 City Road, London EC1V 2PD, UK / Tel: +44-20-7566-2709 / Fax: +44-20-7566-2472 / E-mail: danielelorenzano@hotmail.com
• Received: March 5, 2018 • Revised: July 15, 2018 • Accepted: October 17, 2018
Copyright © 2019 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objective
- To determine whether the use of unique customized spectacles provided with modified side arms may be helpful in reducing benign essential blepharospasm (BEB) in patients describing periocular sensory tricks (ST).
-
Methods
- A prospective descriptive study of patients with BEB with positive periocular or temporal region ST phenomenon response under the care of the Botox Clinic at Moorfields Eye Hospital, London, UK. Nine consecutive patients with BEB describing ST were recruited, and the disease frequency and severity were assessed with the Jankovic Rating Scale (JRS) and the Blepharospasm Disability Index (BSDI) before and after the use of the sensory trick frames (STF).
-
Results
- A reduction in the score was noted in both severity (p = 0.0115) and frequency patterns (p = 0.0117) in the JRS in patients using the STF. A significant reduction of the BSDI score was also observed (p = 0.0314).
-
Conclusion
- All the patients selected and fitted with the STF had a reduction in spasms and related symptoms. This new device may be helpful in some selected BEB patients who previously responded positively to periocular pressure alleviating maneuvers.
- Subjects
- Nine consecutive patients were identified as ST responders from the Moorfields Eye Hospital-Facial Dystonia Clinic. We enrolled 4 females and 5 males, and the mean age of patients was 70 ± 10.3 years. All patients had BEB, four of them were affected by BEB and apraxia, three were affected by BEB only and two had Meige’s Syndrome or BEB associated with adductor laryngeal dystonia. All patients described a significant response to digital pressure alleviating maneuvers applied to specific temporal and lateral periorbital areas. All patients were recruited and evaluated 4 months after the last botulinum injection. Internal institutional approval for the study was obtained from Moorfields Eye Hospital (CA18.AD.123). All patients enrolled in the study signed an informed consent before they were asked to test the STF.
- Each patient had to use the STF for at least 30 days before being interviewed and tested. We encouraged patients to investigate any facial periorbital region that could produce a specific temporary or permanent reduction of the spasms by performing a palpating pressure on the identified triggering areas. An objective demonstration of the effectiveness of the recognized alleviating periorbital maneuver was carried out in the clinic in front of at least two of the doctors taking part in the study, performed in consecutive but separate examinations on the same day. A refractive test was also carried out on all patients enrolled in the study.
- Sensory trick frame kit
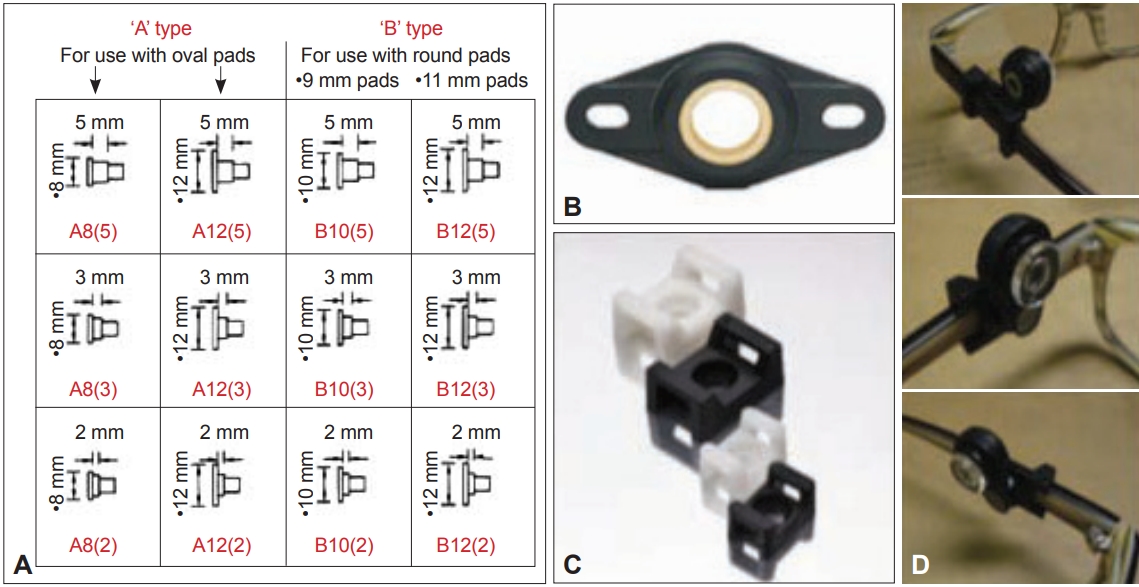
- The blepharospasm STF kit components are produced from off the shelf components that require modifications to enable them to fit to the side arms of certain spectacle frames. These modifications were carried out by the Scientific Workshop Department in the Institute of Ophthalmology–University College London. The spectacle frames are supplied by the Spectacles Dispensing and Manufacturing Department in Moorfields Eye Hospital who also fit the customized assemblies for the patients to apply pressure to their identified effective areas. The components required to set up the frames present a 9.00 mm diameter round silicone nose pads push fit type, an 11.00 mm diameter round silicone nose pads push fit type, both from Accessoreyes Ltd. (Birmingham, UK) (Figure 1A).
- Moreover, an igubal flange (Figure 1B), part number EFOM-04 from Igus® Ltd. (Northampton, UK) and a screw fix cradle (Figure 1C) black, part number CSFM2B from CablecraftTM (Houghton Regis, Dunstable, UK) are modified from their original shape and assembled together. Small plastic mounts, with numerous different sizes and specifications, are produced to mount the nose pads tool. These, in turn, are fitted to the igubal flange that is subsequently fitted to the screw fix cradle. The whole assembly then fits to the spectacle frame arms and can be adjusted along the length of the arms. The igubal flange is modified accordingly to fit to the screw fix cradle. The screw fix cradle is modified to enable it to fit to the spectacle frame arms.
- Spectacles testing
- The patient is asked to report which is the specific temporal and periorbital area that triggers the ST. We ask the patient to identify the specific region addressing how big the ST point is in order to better select the correct nose pad diameter. Moreover, after we have created a first initial ST prototype frame for that specific patient, we continue testing the frame effectiveness by investigating how much pressure needs to be applied on the ST region (Figure 2). For this reason, the patient is required to apply digital pressure on the region starting with a mild pressure and continually increasing the pressure until the spasms are effectively reduced or eliminated. This patient’s subjective active test appears to be able to adequately tailor both the correct localization and specific amount of pressure to achieve an effective spasm reduction or disappearance. The finished spectacle kit components are numbered so that they can be easily identified and replacements can be requested by patients as needed. The completed assemblies, with numerous pressure pad formats and sizes, enable an adjustable system which can be positioned precisely in order to help patients with BEB condition (Figure 1D).
- Clinical assessment
- The evaluation of the efficacy of these spectacles was determined by the severity and frequency of the blepharospasm symptoms which were scored according to the Jankovic Rating Scale (JRS) and the Blepharospasm Disability Index (BSDI). The JRS [10] is a scale which includes two subscales that measure intensity and frequency of eyelid spasms, both based on a 5-point grading system with an excellent internal consistency. The BSDI [11] is a disease-specific patient-rated disability scale that measures impairment of specific activities of daily living caused by blepharospasm. Six items are described in the scale consisting of specified activities (vehicle driving, reading, watching television, shopping, walking, and doing everyday activities), scored as a 5-point scale relating to the severity of impairment. Questionnaires were given to all the patients included in the study and answers were retrieved prior to use of the STF and after 30 days of using the customized STF at a follow up clinic visit. Observation of patients’ behavior with the use of the STF was obtained in the clinic separately by two designated doctors during the whole length of the follow up examination.
- Statistical analysis
- Statistical analysis was performed using SPSS Statistics v 24.0 (IBM Corp., Armonk, NY, USA). Wilcoxon signed-rank test was used to compare the key variables in the data considering pre- and post-JRS [10] severity and frequency scores and pre- and post-BSDI [11] scores.
MATERIALS & METHODS
- All the patients enrolled in the study had to use the STF for at least 30 days before being interviewed and tested using the JRS and the BSDI.
- Jankovic Rating Scale evaluation
- Clear evidence was obtained of a reduction of the JRS scores in both the severity (27 vs. 15 points with no spectacles vs. STF treatment, respectively, Wilcoxon signed-rank test p = 0.0115) and in the frequency scale (27 vs. 17 points with no spectacles vs. STF treatment, respectively, Wilcoxon signed-rank test p = 0.0117). We also performed an overall analysis with severity and frequency assessed together, 54 points prior to treatment vs. 32 points after the STF treatment (Wilcoxon signed-rank test p = 0.0118) which represents a significant improvement in symptoms (Table 1).
- Blepharospasm Disability Index evaluation
- A significant overall reduction of the BSDI was also observed. Changes in scores pre- and post-STF use were noted among all classes considered in the BSDI except for the driving feature. We noted 123 points prior to STF use (13.67 mean, SD 1.87) as opposed to 87 points (9.67 mean, SD 4.44) after the STF treatment (Wilcoxon signed-rank p = 0.0314) (Table 1).
- Table 2 presented 9 patients who showed favorable outcomes in JRS and BSDI.
RESULTS
- At the end of the 1970s Marsden [12] proposed that focal dystonias were neurological entities related to idiopathic torsion dystonia with a possible origin from a basal ganglia disorder. Sensory system abnormalities might have a fundamental part in the pathophysiology of primary late-onset dystonias playing an important role in driving the motor system, as in fact it is recognized that abnormal sensation can lead to disordered movements.
- Factors inducing overload of the sensory system in a certain body areas may explain the emergence of topographically related focal dystonia [13].
- Two different mechanisms have been described to explain ST effectiveness on periocular focal dystonia spasms. One implies that the patients may transiently reduce the spasms by gently touching the periorbital-temporal-facial region, driving a proprioceptive sensory limitation which modulates sensory-motor integration and diminishes abnormal dystonic motor output [6].
- Another mechanism assumes the need for a more energetic type of manual maneuver consisting in performing a forceful counterpressure in opposition to the dystonic periocular muscle contraction. This may be necessary in more severe forms of blepharospasms, where a purely ST may not be sufficient to counteract dystonia [6].
- We assume that a combination approach to address the two mechanisms, due to variations of initial clinical presentation of patients and to diverse underlying pathophysiology mechanisms, may significantly determine the rate of success of the ST maneuver. Moreover, we are aware that the loss of efficacy of ST in a few blepharospasm patients indicates that ST may deteriorate over time.
- The ST or ‘geste antagoniste’ is a well recognized phenomenon [8,10]. Severity and frequency of dystonic movements as in BEB condition are known to be reduced by ST in some patients. Digital ST to specific areas of the face such as the temporal and the periorbital and periocular regions are known to be purposeful maneuvers that temporarily reduce the spasms as long that the pressure is applied. To our knowledge, this is the first study utilizing the alleviating maneuver phenomenon by developing a novel device for improving the symptoms of BEB.
- In our study, we present for the first time a new device for blepharospasm patients who respond to ST digital pressure around the lateral periorbital areas or in the temporal region. The STF mimic effective digital pressure, but they have been recognized to block patient spasms only in those subjects who are already known to be responders to the ST test.
- The various silicone pads and sliding parts have been developed by the Scientific Workshop Department at the Institute of Ophthalmology–University College London, enabling an adjustable system that can be positioned precisely in order to help patients with blepharospasm. Off the shelf frames are modified with the pressure pad formats and sizes in order to enable them to assemble and to fit on to the side arms by our Spectacles Dispensing and Manufacturing Department at Moorfields Eye Hospital.
- Selection of patients is crucial and the triggering areas have to be accurately located and assessed with the patient’s help. We were not able to recognize a specific subtype class of blepharospasm patients that respond better to the use of the STF due to our small study population. Our paper reports an initial case series with a relatively short follow-up. We are aware that both represent limitations to the present study and a longer followup and a larger population in a controlled study design would further explore the effectiveness of this device.
- Nevertheless, our data suggest a novel initial proof of principle demonstrating that the STF device is a unique and useful tool to reduce blepharospasm symptoms in some selected patients. The STF should be considered for use in parallel with conventional blepharospasm therapies as an alternative or to augment treatments, offering further significant improvement.
DISCUSSION
- Dr Ezra receives some funding from the NIHR Biomedical Research Center for Ophthalmology at Moorfields Eye Hospital and University College LondonInstitute of Ophthalmology.
- The blepharospasm spectacle kit components were kindly modified to enable them to fit to the side arms of the Sensory Trick Frames by Paul Johnson and Ian Macartney at the Scientific Workshop Department in the Institute of Ophthalmology–University College London.
Acknowledgments
Figure 1.A: Silicone pressure pad mounts for STF and components and the details of the spectacle pressure pad parts. B: Igubal flange prematching shape. C: Screw fix cradle. D: STF mounted on spectacle arm. STF: sensory trick frame.
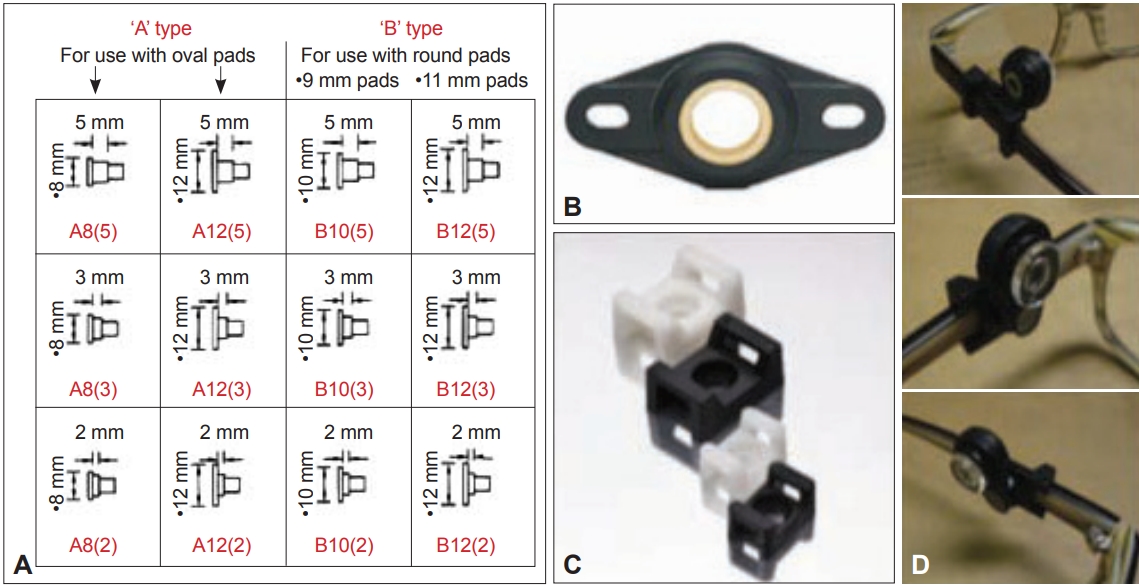

Table 1.Comparison of JRS and BSDI between pre- and post-STF treatment
| Pre-STF scores | Post-STF scores | p† | |
|---|---|---|---|
| JRS severity points | 27 | 15 | 0.0115 |
| JRS frequency points | 27 | 17 | 0.0117 |
| JRS severity + frequency total points | 54 | 32 | 0.0118 |
| BSDI* points | 123 | 87 | 0.0314 |
Table 2.Pre- and post-STF treatment for JRS and BSDI in selected patients
- 1. Kenney C, Jankovic J. Botulinum toxin in the treatment of blepharospasm and hemifacial spasm. J Neural Transm (Vienna) 2008;115:585–591.ArticlePubMedPDF
- 2. Fayers T, Shaw SR, Hau SC, Ezra DG. Changes in corneal aesthesiometry and the sub-basal nerve plexus in benign essential blepharospasm. Br J Ophthalmol 2015;99:1509–1513.ArticlePubMed
- 3. Cohen DA, Savino PJ, Stern MB, Hurtig HI. Botulinum injection therapy for blepharospasm: a review and report of 75 patients. Clin Neuropharmacol 1986;9:415–429.ArticlePubMed
- 4. Albanese A. The clinical expression of primary dystonia. J Neurol 2003;250:1145–1151.ArticlePubMedPDF
- 5. Loyola DP, Camargos S, Maia D, Cardoso F. Sensory tricks in focal dystonia and hemifacial spasm. Eur J Neurol 2013;20:704–707.ArticlePubMed
- 6. Martino D, Liuzzi D, Macerollo A, Aniello MS, Livrea P, Defazio G. The phenomenology of the geste antagoniste in primary blepharospasm and cervical dystonia. Mov Disord 2010;25:407–412.ArticlePubMed
- 7. Greene PE, Bressman S. Exteroceptive and interoceptive stimuli in dystonia. Mov Disord 1998;13:549–551.ArticlePubMed
- 8. Kaji R, Rothwell JC, Katayama M, Ikeda T, Kubori T, Kohara N, et al. Tonic vibration reflex and muscle afferent block in writer’s cramp. Ann Neurol 1995;38:155–162.ArticlePubMed
- 9. Naumann M, Magyar-Lehmann S, Reiners K, Erbguth F, Leenders KL. Sensory tricks in cervical dystonia: perceptual dysbalance of parietal cortex modulates frontal motor programming. Ann Neurol 2000;47:322–328.ArticlePubMed
- 10. Jankovic J, Orman J. Botulinum A toxin for cranial-cervical dystonia: a double-blind, placebo-controlled study. Neurology 1987;37:616–623.ArticlePubMed
- 11. Goertelmeyer S, Brinkmann G, Comes A, Delcker A. The Blepharospasm Disability Index for the assessment of functional health in focal dystonia. Clin Neurophysiol 2002;113:S77–S78.
- 12. Marsden CD. The problem of adult-onset idiopathic torsion dystonia and other isolated dyskinesias in adult life (including blepharospasm, oromandibular dystonia, dystonic writer’s cramp, and torticollis, or axial dystonia). Adv Neurol 1976;14:259–276.PubMed
- 13. Defazio G, Abbruzzese G, Livrea P, Berardelli A. Epidemiology of primary dystonia. Lancet Neurol 2004;3:673–678.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
Citations to this article as recorded by 
- Electrically Induced Sensory Trick in a Patient with Musician’s Dystonia: A Case Report
Daisuke Nishida, Katsuhiro Mizuno, Osamu Takahashi, Meigen Liu, Tetsuya Tsuji
Brain Sciences.2023; 13(2): 223. CrossRef - Evaluation of Blepharoptosis in Patients With Refractory Blepharospasm by VISA—Video Recordings, Idiosyncratic Expressions, Sensory Tricks, and Ancillary Procedures
Chung-Sheng Lai, Savitha Ramachandran, Chia-Chen Lee, Ya-Wei Lai, Yang-Pei Chang, Shu-Hung Huang
Annals of Plastic Surgery.2023; 90(5S): S172. CrossRef - Variability of Movement Disorders: The Influence of Sensation, Action, Cognition, and Emotions
Rok Berlot, John C. Rothwell, Kailash P. Bhatia, Maja Kojović
Movement Disorders.2021; 36(3): 581. CrossRef - Impact of Upper Eyelid Surgery on Symptom Severity and Frequency in Benign Essential Blepharospasm
Hannah Mary Timlin, Kailun Jiang, Daniel George Ezra
Journal of Movement Disorders.2021; 14(1): 53. CrossRef - Benign essential blepharospasm: epidemiology, clinical manifestations, pathophysiology, botulinum toxin therapy
Z. A. Zalyalova
Neurology, Neuropsychiatry, Psychosomatics.2021; 13(1): 119. CrossRef - Best Practices in the Clinical Management of Progressive Supranuclear Palsy and Corticobasal Syndrome: A Consensus Statement of the CurePSP Centers of Care
Brent Bluett, Alexander Y. Pantelyat, Irene Litvan, Farwa Ali, Diana Apetauerova, Danny Bega, Lisa Bloom, James Bower, Adam L. Boxer, Marian L. Dale, Rohit Dhall, Antoine Duquette, Hubert H. Fernandez, Jori E. Fleisher, Murray Grossman, Michael Howell, Di
Frontiers in Neurology.2021;[Epub] CrossRef - Ocular motor manifestations of movement disorders
Grace F. Crotty, Bart K. Chwalisz
Current Opinion in Ophthalmology.2019; 30(6): 443. CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite