Movement Disorders Following Cerebrovascular Lesions: Etiology, Treatment Options and Prognosis
Article information
Abstract
Post-stroke movement disorders are uncommon, but comprise an important part of secondary movement disorders. These exert variable and heterogeneous clinical courses according to the stroke lesion and its temporal relationships. Moreover, the predominant stroke symptoms hinder a proper diagnosis in clinical practice. This article describes the etiology, treatment options and prognosis of post-stroke movement disorders.
INTRODUCTION
Movement disorders are rare, but may present as a consequence of stroke [1,2]. Involuntary movements related to any type of stroke comprise one important part of secondary movement disorders. Post-stroke movement disorders are defined as paroxysmal, recurrent, transient, permanent and delayed movements in the acute phase or as a delayed syndrome occurring months or years after vascular events [1,3]. Thus, movement disorder after stroke is a heterogeneous condition. Abnormal involuntary movements (AIM) following stroke can be classified as hyperkinetic or hypokinetic [4]. Various presentations including tremor, chorea-ballism, dystonia, athetosis, myoclonus, ataxia, and parkinsonism have been associated with vascular brain lesions [1,2,5,6]. The time course for the development of AIM attributed to stroke is not easily predicted, as the course differs according to the type of AIM; they can manifest with a variety of presentations or even in the same movements [4]. Similar to the typical stroke symptoms, the duration of AIM also varies from paroxysmal and/or transient to persistent and progressive [1]. The manifestation of stroke varies even in the same vascular territory [7]. Accordingly, mixed movements are one of the characteristics of secondary AIM associated with a stroke lesion with an extensive involvement. Although the frequency of AIM following stroke is low, it is important to know the possible clinical conditions, its course and symptoms and the proper management strategies, as these aspects could considerably affect a stroke patient’s quality of life as much as the paretic stroke symptoms. This article describes the etiology, treatment options and prognosis of post-stroke movement disorders.
ETIOLOGY OF POST-STROKE MOVEMENT DISORDERS
Stroke lesion location
Post-stroke movement disorders can develop in any stroke subtype and at any brain level of the motor circuit. In the extrapyramidal system, however, the basal ganglia and thalamus are the primary lesion sites associated with post-stroke movement disorders [1,4]. A comparison between stroke patients and case-controls (without movement disorders) revealed that stroke patients with movement disorders feature significantly greater involvement of deep brain lesions affecting the basal ganglia, thalamus, internal capsule, diencephalon, and mesencephalon than stroke patients without movement disorders. Strokes in deep brain lesions are also associated with a higher probability of AIM (odds ratio 3.38, 95% confidence interval 1.64 to 6.99) [1]. For cortical lesions, the areas most commonly associated with post-stroke movement disorders include those involved in the cortical motor system, including the primary motor, supplementary motor and premotor cortical areas. The parietal cortex is also involved in processing somatosensory information related to movement. However, “pure” or “isolated” stroke-related cortical movement disorders are rare, as most “cortical” strokes also affect subcortical structures. Therefore, consideration is needed for the possibility that many “structural” cortical strokes actually have functional defects arising from lesions affecting subcortical structures. Several case reports have described cortical stroke-related movement disorders, including parietal lobe stroke with choreo-ballism [8], focal dystonia [9,10], arm levitation due to distortion of the body schema and athetosis [11]. Frontal lobe stroke is associated with asterixis (negative myoclonus) [7], secondary painless leg moving toe syndrome [12], and resting and action tremor (with strokes affecting the anterior cerebral artery territory) [7,13]. Structural cystic lesions with mass effects of the middle fossa involving the fronto-temporo-parietal area can mimic Holme’s tremor [14]. Alleviation of a previous tremor is also possible after frontal cortical stroke [15]. Some cortical stroke-related movement disorders feature a laterality component: bilateral cortical ptosis can occur with a large right-side, hemispheric lesion [16,17]. Secondary restless legs syndrome (RLS) after stroke has been reported with temporo-occipital cortical lesions, as well as with stroke affecting the basal ganglia, thalamus, internal capsule and pons [18].
Stroke subtypes
A large epidemiologic study previously examined post-stroke movement disorders but was limited by a small number of patients. However, in that study, basal ganglia and thalamus involvement in stroke was frequent [2]. Overwhelmingly, the typical stroke symptoms that occur in the acute phase play a role in overlooking combined movement disorders. In one registry study that enrolled 1,500 consecutive stroke patients, 59 (3.9%) developed post-stroke movement disorders, with chorea as the most common movement disorder subtype [1]. Ischemic stroke can be etiologically classified as a small vessel disease, large vessel disease or cardioembolic stroke [19]. Among the ischemic stroke subtypes, multifocal small vessel stroke is the most commonly associated with movement disorders following stroke, and it is the leading cause of post-stroke AIM. However, cardioembolic stroke and large- and medium-sized atherosclerotic stroke are also included in the etiology of movement disorders [2,20]. Hemorrhagic stroke has a high probability of developing post-stroke movement disorders when compared to ischemic stroke. Generally speaking, there is no specific preference to the vascular region or subtype in post-stroke movement disorders, with only a trend for some of the clinical factors described [21]. Chronic small vessel disease or Binswanger’s disease can develop into secondary parkinsonism (vascular parkinsonism). Vascular parkinsonism is phenomenologically characterized by bilateral slowness and rigidity, which is predominant in the lower extremities, causing gait problems and lower-body parkinsonism [22]. Subcortical small vessel pathology, rather than the typical Lewy body pathology, was reported in the pathologic study of vascular parkinsonism [23].
MOVEMENT DISORDERS IN SPECIFIC STROKE SYNDROMES
CADASIL
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a progressive vascular disease characterized by migraine headache, stroke syndromes, and dementia [24]. CADASIL patients have a variety of movement disorders, including dystonia as an atypical late presentation secondary to chronic ischemic insults. Abnormal findings in dopamine transporter single-photon emission computed tomography imaging without response to dopaminergic treatment has implicated vascular parkinsonism in the CADASIL family [25,26]. Mutations in the NOTCH 3 gene have been reported in potential cases of progressive supranuclear palsy, along with cases of multiple system atrophy with scattered white matter signals [27,28].
MELAS
Mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes (MELAS) syndrome is a distinct clinical syndrome involving skeletal muscles and the brain [29]. As the name suggests, the most common movement disorder in MELAS is myoclonus. Parkinsonism and gait freezing are other symptoms associated with MELAS [30-32]. Nakagaki et al. [33] reported a case of chorea-ballism in MELAS that might accelerate hyperglycemic movement disorders. Although brain lesions in MELAS are not confined to a specific vascular territory [34], the brain pathology might contribute to most of the related secondary movements.
Moyamoya disease
Moyamoya disease is defined by progressive occlusion of the internal carotid artery and arteries in the circle of Willis [35]. Movement disorders in moyamoya disease are rare and have been reported mainly in pediatric patients [36-38]. Regardless of age, the most common AIM in moyamoya disease is chorea [39]. The reported occurrence in one study was 31 of 42 (67.4%) patients, which was followed by dystonia in 8 of 42 (17.4%) patients, with a mean age of onset of 21.4 years [40]. In another study, 5 of 513 pediatric patients with moyamoya disease had AIM, 4 had chorea, and one had dystonia. The symptoms improved in all cases after bypass surgery, suggesting that cerebral ischemia even in the absence of stroke lesions might be a pathogenic mechanism in moyamoya disease [37]. Another retrospective review study of 316 surgically treated children with moyamoya disease reported that 10 (3.2%) children had chorea that resolved following the revascularization surgery. The same authors postulated that dysfunction of the basal ganglia via the hypertrophic collateral vessels was causative for chorea [36].
MANAGEMENT OF POST-STROKE MOVEMENT DISORDERS
Pharmacological treatment
Decisions regarding the management of post-stroke movement disorders should be individualized and based on each clinician’s experience. This reflects the scarcity of case-controlled, randomized clinical trials resulting from the difficulty in collecting appropriate sample sizes. Medical treatment of post-stroke movement disorders is similar to that for primary movement disorders, as they share common underlying pathomechanisms (Table 1). Many cases of post-stroke movement disorders are transient and self-remitting, so no treatment or intervention is needed [41]. Chorea is the most common post-stroke movement disorder [22]. Persistent choreaballism in acute stroke patients needs to be treated, as this might cause significant patient discomfort [3]. Anti-dopaminergic drugs that block the D1 and D2 receptors are the first choice in choreic movements. D3 and D4 receptor antagonists can be used and have the merit of a low risk of extrapyramidal side effects, such as parkinsonism and akinesia. Other atypical neuroleptics should be applied only in refractory cases [5]. Presynaptic dopamine-depleting agents and catecholamine-depleting drugs, as well as GABA receptor agonists, can also be used in selected cases [42]. Consideration for the side effects of each drug is important when choosing a drug for the devastating post-stroke chorea [22]. For post-stroke dystonia, the symptoms rarely improve completely with treatment [43]. Focal injections of botulinum toxin is the usual treatment option, and intrathecal baclofen can be tried for partial symptom relief [5]. Other medical treatments include anticholinergics, baclofen, and benzodiazepam, which is similar to the treatment of primary dystonia. In addition, anti-dopaminergic agents can be tried. Tremor activation in post-stroke tremor disorder is both resting and postural/kinetic [7,13,41]. Although the response to pharmacological treatment of vascular tremors is limited, the treatment options should be decided based on the type of tremor. Of the specific forms of tremor, symptomatic rubral (midbrain) and palatal tremor are usually caused by stroke lesions in the dentate-rubro-thalamic circuits. Limited but potential benefits were reported for propranolol, clonazepam, dopaminergic agents and anti-epileptic drugs, including valproic acid and levetiracetam [22,44]. However, for most refractory cases, surgical intervention and focal botulinum toxin injections are required [45-47]. Post-stroke secondary myoclonus is mostly transient and does not require management. GABAergic drugs (valoproic acid and clonazepam) enhance inhibitory neurotransmission, and levetiracetam and piracetam can be used for symptomatic treatment [48,49]. Some clinicians recommend a combination of these drugs to lessen adverse events. Vascular parkinsonism is characterized by symmetric akinesia and gait impairment [50,51]. The effect of representative treatment with levodopa for vascular parkinsonism may be poor and short-lasting [1,3]. Post-stroke RLS is not uncommon in the acute stroke phase (17 out of 137 cases) and has been associated with dysfunction of the subcortical dopaminergic system of the basal ganglia and thalamus [18,52]. Secondary RLS associated with acute stroke is mostly transient and improves without medication. When treatment is required, dopaminergic agents might help to relieve symptoms [18]. Treatment of post-stroke tics is the same as with primary tics: clonidine, neuroleptics, dopaminedepleting agents can be applied [53].
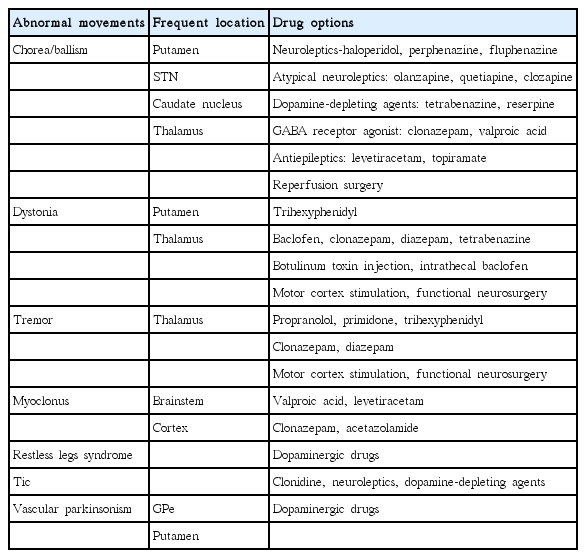
Representative treatment options for post-stroke movement disorders
Surgical treatment
In drug-resistant and devastating post-stroke movement disorders, surgical intervention can be considered. For secondary movement disorders caused by vascular hypoperfusion of the carotid or vertebrobasilar artery, revascularization surgery may result in near complete symptom improvement [54-58]. Chronic motor cortex stimulation was originally used for post-stroke pain control, but effective control of involuntary movements (choreo-athetosis, action and resting tremor) can also be obtained [59]. Several mechanisms of action, including hyperdirect motor cortex-subthalamic nucleus input, cortical inhibition, and plastic changes, have been proposed for motor cortex stimulation in various movement disorders [60]. Movement disorders attributed to moyamoya syndrome can be improved through bypass surgery [38]. Deep brain stimulation (DBS) targeting the globus pallidus and thalamic nucleus (nucleus ventralis oralis posterior, nucleus ventralis intermedius) are other useful options for treating drug-refractory chorea and/or dystonia [5,43,61,62]. Pallidotomy, thalamotomy and DBS of the thalamus in patients with severe tremor, including a high amplitude and low frequency, are several treatment options worth trying for symptomatic control [5,45].
Physical therapy and rehabilitation
Proper rehabilitation is needed for most stroke patients [63]. Physical and occupational therapy have become important assistive therapeutic options for secondary movement disorders. Physical therapy is helpful for both hypokinetic and hyperkinetic movement disorders, such as vascular parkinsonism and dystonia, which are associated with postural deformity and balance problems [64,65]. Physical therapy and brace devices [3,5], as well as proprioceptive rehabilitation [66], may be applied for movement disorders after stroke.
PROGNOSIS OF POST-STROKE MOVEMENT DISORDERS
Onset latency
Many of the post-stroke movement disorders develop during the acute phase, especially within several days of the stroke onset. The timing can cause clinicians to overlook and under-diagnose the presence of post-stroke movement disorders because of the overwhelming motor and sensory deficits [1]. The clinical course of post-stroke movement disorders is variable, but some tendencies are apparent according to which type of AIM is presented [3]. The period for developing a movement disorder after stroke is between the stroke onset to years after the onset [1,2]. The latency interval of post-stroke movement disorders is shortest for chorea (4.3 days) and longest for parkinsonism (117.5 days) [1]. Transient hemichorea-ballism can develop even before stroke in the form of transient ischemic attacks and can serve as a warning sign [67-69]. Post-stroke RLS can appear within a week after the onset of stroke (mean 1.8 days) [18].
Long term prognosis
Most of the post-stroke movement disorders typically have a short duration and improve over time. Among the post-stroke movement disorder subtypes, chorea, myoclonus, and especially asterixis, do not last long and are self-limiting. Vascular parkinsonism tends to persist and progressively deteriorates [1]. Dystonia also has a poor prognosis with significantly worsened activities of daily living and quality of life. Tremor, especially symptomatic cerebellar-outflow tremor with low frequency, persists and worsens, and it is specifically refractory to medical treatment [5].
CONCLUSIONS
Post-stroke movement disorders are rare, but they account for an important part of secondary AIM. Various manifestations of hyperkinetic and hypokinetic movements, as well as overwhelming stroke symptoms, make timely diagnosis of combined movement disorders challenging. Any stroke lesion occurring in the motor system from the cortex to brainstem, any etiologic subtype of stroke, regardless of the lesion size, and a variety of systemic syndromes that can cause stroke may cause involuntary movement. Therefore, clinicians should consider the possibilities associated with AIM when treating acute stroke patients in clinical practice. Concerning the clinical course, most post-stroke movement symptoms are transient and self-limiting. However, proper diagnosis with a treatment strategy is critical because sometimes these might persist and become life-threatening with significant detriment to the victim’s quality of life. Timely treatment could hasten the recovery and prevent a worsening of symptoms. Although there are no established treatment guidelines based on randomized case-controlled studies, which reflects the low prevalence of these disorders, most of the pharmacological treatment options for secondary movements are not dissimilar to those for primary movement disorders based on similar underlying pathomechanisms. The treatment strategies include controlling dopaminergic excitability and modulating GABAergic transmission. Catecholamine-depletion and anti-cholinergic drugs are other options used to control AIM. Recently, symptomatic control with botulinum toxin injections, which blocks peripheral release of acetylcholine at the muscle level or intrathecal baclofen infusion, has been introduced as a therapeutic option for drug-resistant post-stroke dystonia. Repeated transcranial magnetic stimulation is another useful treatment option in limited cases of drug-resistant secondary dystonia and tremor. In cases of irresistible post-stroke movement disorder, surgical intervention might be considered. Exercise and physical therapy should always be considered to achieve better outcomes.
Notes
Conflicts of Interest
The author has no financial conflicts of interest.