Predominant Jaw Myoclonus from Cefepime Toxicity: A Case Report and a Review of the Literature
Article information
Dear Sir,
Cefepime is a commonly prescribed antibiotic, but the frequency and incidence of its neurotoxicity are unknown [1]. Common symptoms of neurotoxicity include lethargy, confusion, agitation, global aphasia, seizures, coma, and myoclonus [2]. Early discontinuation after the development of neurotoxicity is crucial to recovery and to reducing morbidity and mortality [3]. The pathophysiology of cefepime-induced myoclonus is unknown. Much of the current literature does not describe debilitating jaw myoclonus [1,3-6]. Here, we expand on our two previously-reported cases of cefepime-induced jaw myoclonus [7] and introduce a new case. As in the first two cases, this case had varying degrees of renal and cardiac dysfunction [7] contributing to symptom development. Although other antibiotics were used, the resolution of symptoms after cefepime discontinuation makes it the likely cause.
An 88-year-old man presented to the emergency room with shortness of breath. On admission, his temperature was 99.8 degrees Fahrenheit and his blood pressure was 80/30. The neurological examination was non-focal. His chest radiograph revealed a right apical infiltrate, and he was admitted with presumed pneumonia. He was given 2 grams of cefepime by intravenous (IV) daily. In addition, he was given single doses of 400 mg moxifloxacin, 360 mg gentamicin, and 1,250 mg vancomycin in the emergency room by IV. An IV of 500 mg metronidazole every 8 hours was subsequently added and continued until discharge. His creatinine and blood urea nitrogen at the time of admission were 1.7 mg/dL and 27 mg/dL, respectively and remained stable during his hospitalization. His calculated glomerular filtration rate (GFR) was 35 mL/min/1.73 m2 . Echocardiogram demonstrated an ejection fraction of 35 percent. On day three of the admission, he had transient bilateral upper extremity jerking. On day four, he had persistent myoclonus of the entire face, most prominently of his mouth and jaw, extending to the left side of the trapezius, with a frequency greater than 1 hertz. He was awake and communicative but disoriented with regard to place and time. Head CT and EEG were not performed, based on our prior experience from our two previously reported cases [7]. Cefepime was immediately stopped and replaced with ceftriaxone. His jaw myoclonus ceased, and his mental status improved the next day. Cefepime is a fourth-generation cephalosporin, commonly prescribed because of its broad coverage. Its half-life is two hours in patients with normal renal function. Because it is mainly eliminated by glomerular filtration, its serum levels increase with kidney injury. Our case further demonstrates that despite appropriate renal dosing, in the case of kidney injury, myoclonus developed due to cefepime, as illustrated by the resolution of symptoms following its discontinuation. We performed a PUBMED search, focusing on articles in English, using the terms, “cefepime and myoclonus,” “cefepime and neurotoxicity,” and “cefepime encephalopathy” and identified 22 cases of cefepime-induced myoclonus (Table 1) [1,3-7]. As in our case, all 22 of the previous cases [1,3-7] had varying degrees of renal impairment. Age is also an important risk factor because 18 of 22 reported cases were 65 years of age or older. Taken together, age and underlying kidney disease were highly associated with cefepime-induced myoclonus. Renal mass, renal plasma flow, and GFR all decline with age but may not result in an increase in plasma creatinine because of the loss of muscle mass in the elderly. Decreases in renal function affect the clearance of water-soluble antibiotics, such as cefepime, leading to toxic serum concentrations. In addition, patients with underlying kidney injury have elevated serum urea, which leads to an increased permeability of the blood brain barrier, further predisposing patients to neurotoxicity [2]. Multiple comorbidities, underlying infection, and drug polypharmacy appear to be other contributing factors [1,3-7]. Although physiologic changes contribute to the development of antibiotic-induced myoclonus, cephalosporins may inherently reduce GABAergic activity by inhibiting the binding of GABA to GABA-A receptors, resulting in neuronal hyperexcitation and epileptogenicity [2]. Another proposed mechanism of cephalosporininduced neurotoxicity is its induction of endotoxins and the release of cytokines [2].
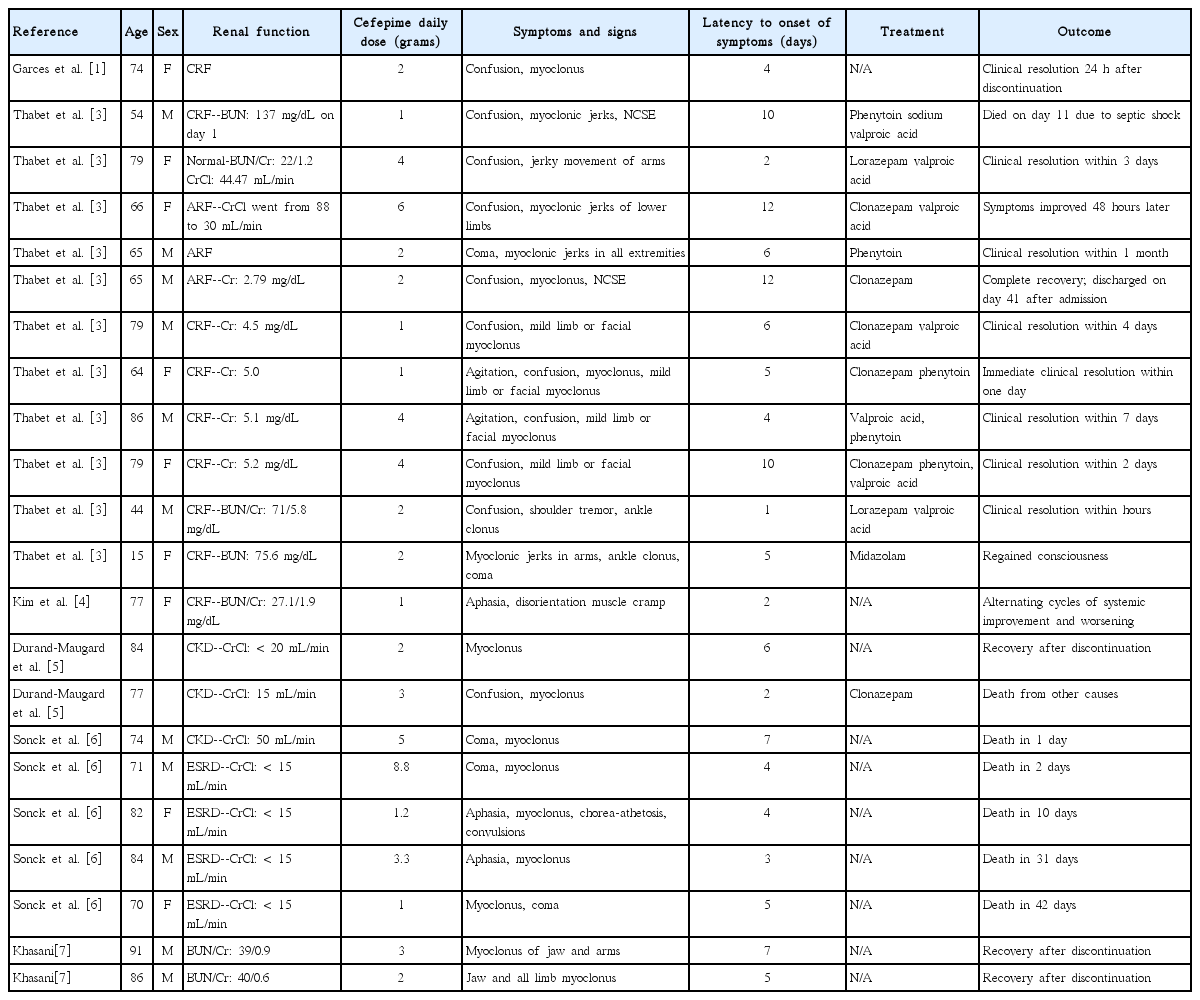
Clinical characteristics of previously reported cases of cefepime-induced myoclonus
It is not entirely clear why the jaw in particular was so severely affected because it is not a well-described phenomenon in cases of antibiotic-induced myoclonus. Although, based on the resolution of symptoms after its discontinuation, cefepime is the likely causative agent, it should be noted that the other antibiotics used to treat our patients have potential neurotoxic effects [2]. Prolonged use of metronidazole has been shown to cause T2 MRI changes in the cerebellum and brainstem, manifesting as limb and gait ataxia, dysarthria, dizziness, headache, confusion, and peripheral neuropathy [2]. Although the rapid resolution of symptoms after discontinuation (within three to seven days) is similar to cefepime, the latency to the onset of symptoms is much longer (up to three months after metronidazole initiation) [2]. In our patient, who was on both metronidazole and cefepime, the latency to the onset of symptoms was only 5 days, unlike previously reported cases of metronidazole-induced neurotoxicity [2]. Furthermore, the myoclonus resolved after discontinuing cefepime, despite the continuation of metronidazole treatment, suggesting that cefepime was the culprit.
In patients with impaired renal function, dose adjustment of cefepime must be performed before drug administration, and patients must be closely monitored for any neurological change. When suspecting neurotoxicity, cefepime should be immediately discontinued and cefepime serum concentrations as well as renal function should be monitored. There is evidence of improvement with decreasing serum cefepime concentrations [5]. Our patient did not have his serum cefepime levels measured due to the resolution of his symptoms upon discontinuation. In our opinion, EEG and neuroimaging are generally recommended to assess for possible underlying electrical and structural causes of myoclonus, especially if there is no resolution with the discontinuation of cefepime. Prescription of anti-epileptics, such as valproic acid, levetiracetam, and clonazepam, as well as hemodialysis for nephrotoxicity aid in treatment [2].
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.