1Neurology and Neurosurgery Discipline of Medicine School, State University of West Paraná (Unioeste), Cascavel, Paraná, Brazil
2Neuroclinica Cascavel, Paraná, Brazil
Corresponding author: Paulo Eduardo Mestrinelli Carrilho, MD, MSc Neurology and Neurosurgery Discipline of Medicine School, State University of West Paraná (Unioeste), 925 Santa Catarina st., Cascavel, Paraná 85813410, Brazil / Tel: +55-4530380297 / Fax: +55-45999718282 / E-mail: pemcarrilho@gmail.com
This case report was presented during a poster session of the XVIII Brazilian Meeting of Neurology, 2018.
• Received: February 17, 2020 • Revised: March 11, 2020 • Accepted: March 31, 2020
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Cerebral disorders are well-known causes of dyskinesias that can mimic myoclonus, but spinal and peripheral nerve diseases have received little attention as causative factors in movement disorders. A variety of peripheral nerve and spinal cord lesions are associated with focal myoclonus. These include peripheral nerve tumors, traumatic injury, radiation damage, spinal cord trauma, spinal tumors, vascular lesions and inflammatory or demyelinating spinal cord diseases [1]. Muscle spasms can even occur in amputation stumps [2]. Symptomatic myoclonus is present in approximately 20% of patients with spinal lesions or neuroinfections, patients taking different kinds of medications and even in patients with paraneoplastic diseases [1]. Myoclonic jerking of the paraspinal muscles due to malignant tumors involving thoracic roots and focal myoclonus after lumbar laminectomy or lumbosacral radiculopathy, electric injury to the brachial plexus or other kinds of peripheral nervous system damage is also, but rarely, a well-known entity [1,2]. Even extrinsic peripheral nerve compression can be associated with focal muscle spasm [3,4]. The present article presents an unusual form of dorsal muscle spasm after spinal surgery for removal of a benign schwannoma. The case was a Brazilian female of japanese origin who was 63 years of age and who did not have major health problems. The patient signed a consent form to allow the use of her clinical and image data for scientific purposes. She had previously developed a three-month history of dorsal pain, which motivated a neurological evaluation where profound bilateral patellar and aquilian hyperreflexia and a left Babinski sign were noticed, in addition to the reported interscapular pain. No motor deficits were noticed, and no involuntary movements were present. The initial complementary investigation with magnetic resonance imaging (MRI) revealed an intradural tumor at the level of T3 (Figure 1A). She underwent tumor removal, which histologically confirmed a schwannoma. The surgery was a successful routine laminotomy from T2 to T4, without major complications, and her postsurgery condition was unremarkable. Recently, a new MRI scan also demonstrated complete removal of the tumor (Figure 1B). Only 6 months later, she started to feel that her dorsal surgery scar developed some kind of involuntary movement, which she felt was described by “twitching” and “dancing” without her control. Her neurological exam revealed focal myoclonus- like movements of the scar, with spasms of the bilateral trapezius and paravertebral muscles (Supplementary Video 1 in the online-only Data Supplement), which remained during sleep. The rest of the neurologic exam was normal, and she had no other complaints, with the exception of the discomfort regarding the feelings of dorsal muscle jerking. A psychological evaluation had not disclosed any major problems and the movements were noticed even during sleep. The initial treatment was a gabapentin trial, without a clear benefit. Later, treatment with onabotulinum toxin A guided by electromyography promoted a transient improvement in her clinical condition.
A “twitching scar” after an uncomplicated facial surgery can be devastating for plastic surgeons. This term was created in 1971 by Converse and Coburn5 to describe two patients who had developed muscle spasms around the surgery scar after rhytidoplasty (face-lift) in one patient and after surgery to treat a small laceration over the zygomatic arch in the other patient. In the literature, there is an extensive list of movement disorders with involuntary muscle twitches or spasms reported after peripheral trauma and surgery [3]. Different types of muscle spasms of the paraspinal muscles due to tumors addressing spinal roots and focal myoclonus after laminectomy or lumbosacral radiculopathy can be included in this list.1
The patient presented in this article had a quaint form of dyskinesia, and a multifactorial origin is associated with the arrival of the unusual muscle spams. Based merely on the clinical impression, the observed involuntary movements strongly resembled a myoclonic disorder, but as no electromyography study was obtained, it was not possible to confirm that this symptom was actually myoclonic jerking. Even a psychogenic movement disorder was considered, but the psychiatric evaluation was completely normal. Furthermore, the muscle spasms continued during sleep, which is uncommon in this specific entity. We strongly believed that myoclonus was more suitable for definning the dyskinesia observed.
Myoclonus is defined as a sudden muscular contraction that usually indicates disease of the central nervous system and may be cortical, subcortical, or spinal in origin. Spinal myoclonus is a rare disorder characterized by myoclonic movements in muscles that originate from several segments of the spinal cord [2]. Spinal myoclonus has been associated with laminectomy, remote effects of cancer, spinal cord injury, postoperative pseudomeningocele, laparotomy, thoracic sympathectomy, poliomyelitis, herpes myelitis, lumbosacral radiculopathy, spinal extradural block, myelopathy due to demyelination, electrical injury, acquired immunodeficiency syndrome, and cervical spondylosis [1,2]. On rare occasions, spinal myoclonus can be observed after peripheral nerve lesions [3]. It is well known that compression of the facial nerve by a cerebellopontine angle mass lesion or by aberrant arteries in the posterior fossa can produce repetitive clonic and tonic contractions of one side of the face. Such conditions can be observed after Bell’s palsy as a late complication [4,6,7].
Although structural lesions are usually found in myoclonus associated with spinal disorders, the pathophysiology remains speculative. Various possible mechanisms can be involved: loss of inhibitory function of local dorsal horn interneurons, abnormal hyperactivity of local anterior horn neurons, aberrant local axon re-excitations and loss of inhibition from suprasegmental descending pathways [1,2]. In the present case, perhaps the simple manipulation of both spinal and peripheral nerves during surgery associated with highly chronic changes in the spine related to schwannoma may be implicated. Other suggested mechanism may be the local irritation of peripheral nerves, promoting ectopic excitation and ephatic transmissions, perhaps associated with traumatic demyelination during surgery [6]. Moreover, as it was a late manifestation in the present case, perhaps abnormal branching after aberrant axonal regeneration and enhanced motor neural excitability could be possible explanations of this disorder [6,7]. Further, a post-mortem study may eventually help in defining histologic abnormalities in the spine, roots and/or peripheral nerves, with the aim of supporting these ideas.
It is important to note that no clear surgical “extra” damage occurred, and no tumor relapse was detected in the present case (Figure 1). Notably many muscles with spasms were not included in the same myotomes directly involved by the tumor or by the surgery. In this sense, it is possible to consider that minimal and non-perceived damage to the peripheral nerves, probably related to the manipulation of muscles and nerves during surgery, could be one of the sources of this unusual dyskinesia.
In conclusion, despite being an exceedingly rare phenomenon, focal or segmental muscle spasms such as myoclonic jerking could be an uncommon manifestation after routine and “uncomplicated” spine surgery, as we pointed out in this very peculiar and interesting case.
Video 1. Muscles twitches related to the surgery scar. The patient described as it was like a “dancing scar.”
Notes
Conflicts of Interest
The authors have no financial conflicts of interest.
Author Contributions
Conceptualization: Paulo Eduardo Mestrinelli Carrilho. Data curation: Paulo Eduardo Mestrinelli Carrilho. Formal analysis: Paulo Eduardo Mestrinelli Carrilho. Funding acquisition: Paulo Eduardo Mestrinelli Carrilho. Investigation: all authors. Methodology: Paulo Eduardo Mestrinelli Carrilho. Project administration: all authors. Resources: all authors. Software: Paulo Eduardo Mestrinelli Carrilho. Supervision: Marcius Benigno Marques dos Santos. Validation: Paulo Eduardo Mestrinelli Carrilho. Visualization: Marcius Benigno Marques dos Santos. Writing—original draft: Paulo Eduardo Mestrinelli Carrilho. Writing—review & editing: Paulo Eduardo Mestrinelli Carrilho.
Acknowledgments
None.
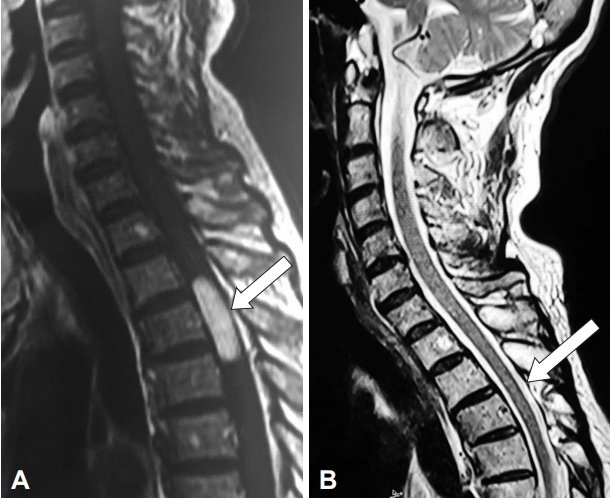
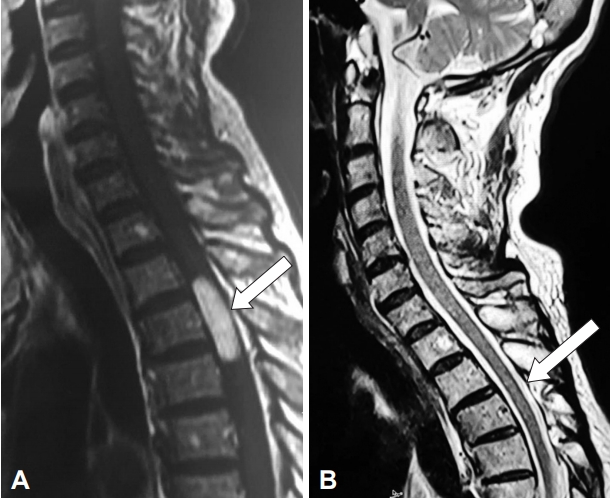
Figure 1.
Magnetic resonance imaging fluid-attenuated inversion recovery (FLAIR) and T2 sequence disclosing T3 level spine schwannoma (arrows). A: Pre surgery. B: Post surgery.
REFERENCES
1. Jankovic J, Pardo R. Segmental myoclonus. Clinical and pharmacologic study. Arch Neurol 1986;43:1025–1031.ArticlePubMed
2. Di Lazzaro V, Restuccia D, Nardone R, Oliviero A, Profice P, Insola A, et al. Changes in spinal cord excitability in a patient with rhythmic segmental myoclonus. J Neurol Neurosurg Psychiatry 1996;61:641–644.ArticlePubMedPMC
3. Savrun FK, Uluduz D, Erkol G, Kiziltan ME. Spinal myoclonus following a peripheral nerve injury: a case report. J Brachial Plex Peripher Nerve Inj 2008;3:18.ArticlePubMedPMCPDF
4. Carrilho PE, Paula CF, Soares EW, Alves O. Focal facial spasms associated with benign parotid hypertrophy. Arq Neuropsiquiatr 2008;66:83–84.ArticlePubMedPDF
6. Nielsen VK. Pathophysiology of hemifacial spasm: I. Ephaptic transmission and ectopic excitation. Neurology 1984;34:418–426.ArticlePubMed
7. Valls-Solé J, Montero J. Movement disorders in patients with peripheral facial palsy. Mov Disord 2003;18:1424–1435.ArticlePubMed
Figure & Data
References
Citations
Citations to this article as recorded by
Pain After Spine Fusion for Adolescent Idiopathic Scoliosis Manaf H. Younis, Adam L. Haydel, Lauren Saunee, Rutledge C. Clement Journal of the Pediatric Orthopaedic Society of North America.2022; 4(2): 381. CrossRef
 E-submission
E-submission
 , Marcius Benigno Marques dos Santos1,2
, Marcius Benigno Marques dos Santos1,2
 PubReader
PubReader ePub Link
ePub Link Cite
Cite