 E-submission
E-submission
Articles
- Page Path
- HOME > J Mov Disord > Volume 12(1); 2019 > Article
-
Original Article
The ‘Hot Cross Bun’ Sign Is Not Always Multiple System Atrophy: Etiologies of 11 Cases -
Christopher Way1
 , David Pettersson2, Amie Hiller3,4
, David Pettersson2, Amie Hiller3,4 -
Journal of Movement Disorders 2019;12(1):27-30.
DOI: https://doi.org/10.14802/jmd.18031
Published online: December 19, 2018
1Parkinson’s Institute and Clinical Center, Sunnyvale, CA, USA
2Department of Diagnostic Radiology, Neuroradiology, Oregon Health & Sciences University, Portland, OR, USA
3Department of Neurology, Movement Disorders, Portland Veterans Administration, Parkinson’s Disease Research, Education and Clinical Center, Portland, OR, USA
4Department of Neurology, Parkinson Center & Movement Disorders Program, Oregon Health & Sciences University, Portland, OR, USA
- Corresponding author: Christopher Way, DO, https://orcid.org/0000-0002-2236-9832 Parkinson’s Institute and Clinical Center, 675 Almanor Avenue, Sunnyvale, CA 94085, USA / Tel: +1-408-734-2800 / Fax: +1-408-734-9208 / E-mail: cway@parkinsonsinstitute.org
Copyright © 2019 The Korean Movement Disorder Society
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ABSTRACT
-
Objective
- To clarify the specificity of the ‘hot cross bun’ sign (HCBS) for multiple system atrophy (MSA) in adult cerebellar ataxia or parkinsonism.
-
Methods
- The radiologic information systems at an academic center and affiliated veterans’ hospital were queried using the keywords ‘hot cross bun,’ ‘pontocerebellar,’ ‘cruciate,’ ‘cruciform,’ ‘MSA,’ ‘multiple system atrophy,’ and ‘multisystem atrophy.’ Scans were reviewed by a neurologist and neuroradiologist to identify the HCBS. Subjects with the HCBS were reviewed by 2 neurologists to identify the most likely etiology of the patient’s neurologic symptoms.
-
Results
- Eleven cases were identified. Etiologies included MSA (4 probable, 2 possible), hereditary cerebellar ataxia (3/11), probable dementia with Lewy bodies (1/11), and uncertain despite autopsy (1/11).
-
Conclusion
- MSA was the most common etiology. However, 5 of the 11 patients did not have MSA. The most common alternate etiology was an undefined hereditary cerebellar ataxia (3/11).
- The radiologic information systems at a single academic institution and an affiliated veterans hospital were queried to identify brain MRI radiology reports from January 2000 to February 2017 containing the terms ‘hot cross bun,’ ‘pontocerebellar,’ ‘cruciate,’ ‘cruciform,’ ‘MSA,’ ‘multiple system atrophy,’ and ‘multisystem atrophy.’ A movement-disorder neurologist reviewed the MRI reports or scans and excluded all subjects that did not have the HCBS or a description consistent with it. A neuroradiologist reviewed the scans that were not excluded to confirm the presence of the HCBS.
- The medical records of all included subjects were reviewed separately by 2 movement-disorder neurologists to determine the most likely causative etiology of the HCBS. Cases not consistent with a typical presentation of MSA with adult (age of onset > 30 years of age) cerebellar ataxia or parkinsonism were excluded. If there was a diagnosis from autopsy or genetic testing that accounted for the patient’s clinical picture, this was accepted as the etiology. The medical record was reviewed for the clinical, laboratory, and imaging data that might support a specific etiology. Parkinsonism was defined as bradykinesia with rigidity, tremor, or postural instability. A cerebellar syndrome was defined as gait ataxia with cerebellar dysarthria, limb ataxia, or cerebellar oculomotor dysfunction. If the information was not documented, it was assumed to be absent. These data were used to determine if the subject met the criteria for probable or possible MSA according to the Second Consensus Statement [8]. Both neurologists then met to review each case and agree upon a neurological diagnosis as the etiology of the HCBS based upon the documented clinical data.
- The study was approved by the Oregon Health & Science University (eIRB #16731) and Portland Veterans Administration (MIRB #4050) Joint Institutional Review Board. A waiver of Informed consent process and authorization was obtained.
MATERIALS & METHODS
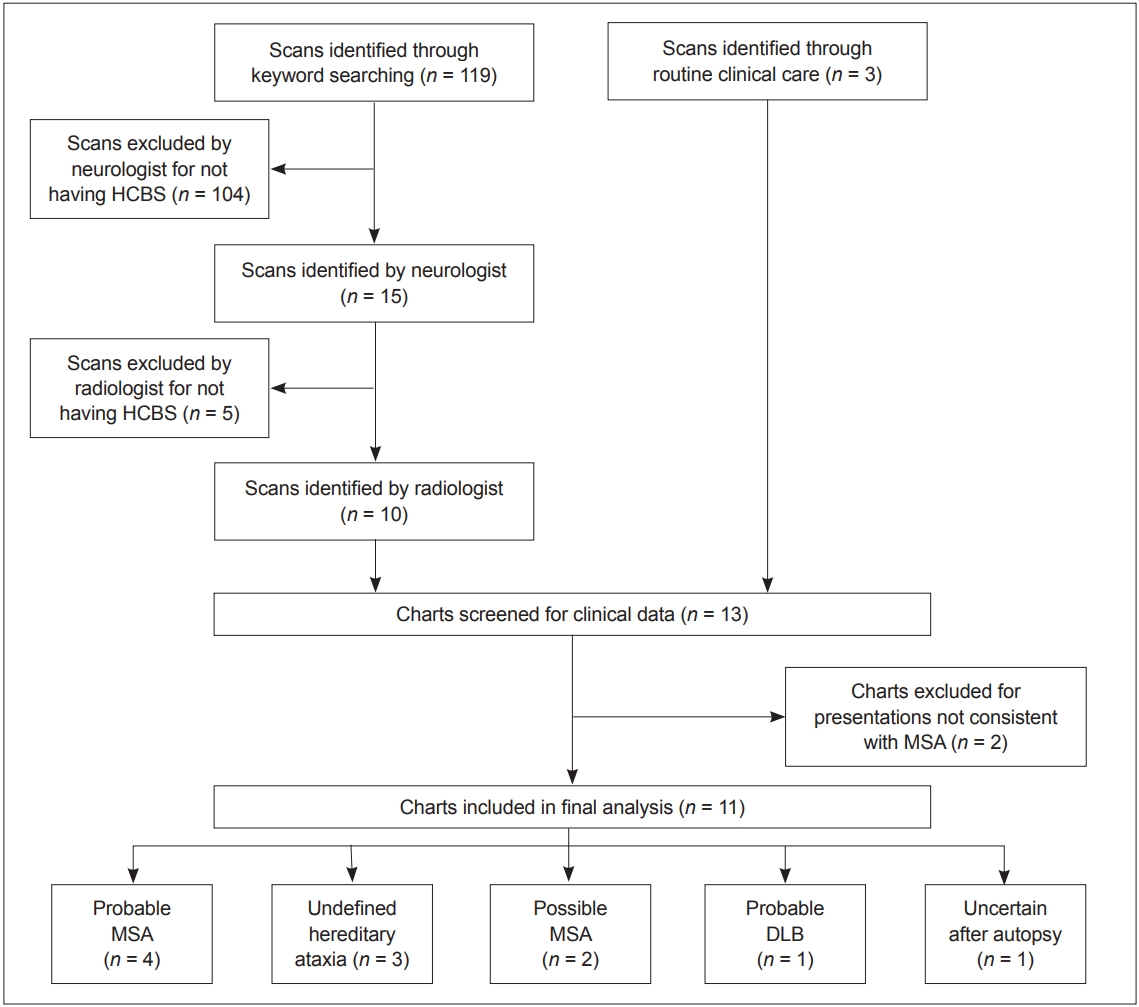
- The initial keyword search identified 119 patients whose radiology reports contained at least one of the search keywords. Further review of these radiology reports and the associated MR images found that 10 of 119 patients had MR imaging positive for the HCBS. Two of 10 patients with a HCBS were not consistent with adult cerebellar ataxia or parkinsonism and were excluded. These consisted of a childhood case of congenital olivopontocerebellar atrophy and an adult case that presented with cognitive impairment. Three cases with the HCBS discovered during routine clinical practice were included after the database search had taken place. Ultimately, 11 cases were included in the analysis. Figure 1 outlines the process utilized for subject inclusion.
- Brain tissue with pathology analysis was available for only 1 case. In life, this patient (case 2) had freezing of gait, rigidity, sialorrhea, and dysphagia suggestive of MSA; however, at autopsy there was only mild loss of pigmented neurons in the substantia nigra and negative staining for alpha-synuclein. There were no glial cytoplasmic inclusions. The case was reviewed by a neuropathologist who confirmed that the autopsy was not consistent with MSA. Genetic testing was negative for SCA1, 2, 3, 6, 7, 8, 10, and 17, dentatorubral-pallidoluysian atrophy, and Friedrich’s ataxia. This subject’s diagnosis was uncertain despite autopsy.
- Genetic testing was performed in 2 of the remaining cases and was negative in both (cases 5 and 11). Patient 5 developed dysarthria and gait imbalance at age 36. Her oldest son and brother had global developmental delay, and her youngest son and niece had epilepsy. Testing for SCA1, 2, 3, 6, and 7 was negative. Due to urinary urgency and orthostatic hypotension, she fulfilled the clinical criteria for possible MSA. However, since the young age of onset and positive family history were atypical of MSA, her clinician suspected an undefined SCA, and this case was labeled as ‘undefined hereditary ataxia’. Cases 10 and 11 were 2 slowly progressive young-onset progressive cerebellar ataxias with family histories supporting an autosomal dominant inheritance pattern. Patient 10 did not have genetic testing, and patient 11 was negative for SCA1, 2, 3, 6, 8, and 17, but due to high clinical suspicion, both of these cases were diagnosed as ‘undefined hereditary ataxia’.
- Patient 3 developed progressive cognitive decline and hallucinations at age 60. There was no orthostatic hypotension, erectile dysfunction, dysphagia, or urinary frequency or incontinence. Parkinsonism with antecollis was noted at age 64. At age 65, he had fluctuating cognitive impairment and scored 18/30 on Mini-Mental State Examination. He fulfilled the clinical criteria for probable dementia with Lewy bodies.
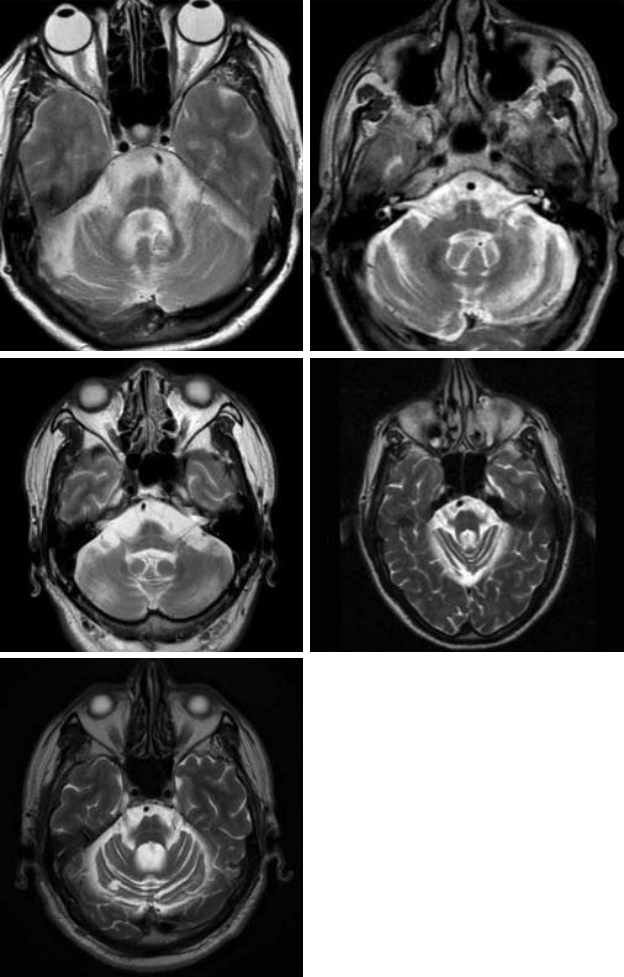
- Of the remaining 6 cases, 4 met the clinical criteria for ‘probable MSA’ and 2 for ‘possible MSA’. Figure 2 displays axial T2 sequences of the pons of the non-MSA subjects with the ‘hot cross bun’ sign. Table 1 summarizes the clinical characteristics of the subjects with the HCBS.
RESULTS
- Current literature describes the HCBS as ‘highly specific for MSA.’ [9] This may lead clinicians to prematurely diagnose patients with MSA based upon the presence of an HCBS. In our sample, the HCBS clearly influenced the clinician to code a diagnosis of MSA in 3 of 11 cases.
- Fiber tractography in a clinically probable MSA-C case with the HCBS has shown decreased volume of fiber bundles corresponding to the corticospinal tracts, transverse pontocerebellar fibers, pons, and cerebellum compared to a healthy subject [10]. We hypothesized that any cause of pontocerebellar degeneration would result in the HCBS and that MSA would be the most common, but not the only, etiology of this sign.
- We included all subjects presenting clinically with adult cerebellar ataxia or parkinsonism at our centers found to have the HCBS, with the aim of clarifying the specificity of the sign for MSA in a sample with a conceivable age range and initial symptomatology for MSA. Six of the 11 subjects met the Second Consensus Criteria for probable or possible MSA. Although only 1 of the 5 non-MSA patients had an autopsy, the remaining subjects had clinical presentations that were very atypical of MSA. This suggests that the HCBS is not as specific for MSA as has been described. However, it is worth noting that 3/5 of the non-MSA patients had symptom onset in their 30s, and of the patients with age of onset > 50 years, 6/8 were diagnosed with probable or possible MSA.
- There are some limitations to this study. There were no genetically confirmed ataxia cases. Of the 3 cases labeled as ‘hereditary ataxia,’ the etiologies were not specifically defined, though the onset in the 4th decade of slowly progressive cerebellar ataxias with autosomal dominant family histories strongly supports an undefined hereditary ataxia. Similarly, none of the MSA cases were pathologically confirmed, and the diagnoses were made solely based on the Second Consensus Criteria. Without genetic or postmortem verification, there may have been some misdiagnoses in the clinically diagnosed cases.
- In addition, the keyword search could only search internal MRI reports, and cases of the HCBS that had MRIs reviewed by outside radiologists prior to referral to our center may have been missed. This was likely a significant factor limiting the sample size of our study.
- In our sample, the HCBS was not specific for MSA, with only 6/11 of the cases fulfilling the clinical criteria for probable or possible MSA. A larger study with pathologic confirmation needs to be performed to further clarify the specificity of the HCBS for MSA.
DISCUSSION
- 1. Lee YC, Liu CS, Wu HM, Wang PS, Chang MH, Soong BW. The ‘hot cross bun’ sign in the patients with spinocerebellar ataxia. Eur J Neurol 2009;16:513–516.ArticlePubMed
- 2. Jain RS, Nagpal K, Tejwani S. ‘Hot-cross bun’ and ‘inverse trident sign’ in progressive multifocal leukoencephalopathy with HIV seropositivity. Neurol India 2014;62:341–342.ArticlePubMed
- 3. Ishikawa H, Kawada N, Taniguchi A, Odachi K, Mizutani A, Asahi M, et al. Paraneoplastic neurological syndrome due to burned-out testicular tumor showing hot cross-bun sign. Acta Neurol Scand 2016;133:398–402.ArticlePubMed
- 4. Pan Z, Yang G, Yuan T, Wang Y, Pang X, Gao Y, et al. ‘Hot cross bun’ sign with leptomeningeal metastases of breast cancer: a case report and review of the literature. World J Surg Oncol 2015;13:43.ArticlePubMedPMCPDF
- 5. Roh SY, Jang HS, Kim YH. Hot cross bun sign following bilateral pontine infarction: a case report. J Mov Disord 2013;6:37–39.ArticlePubMedPMCPDF
- 6. Jain RS, Sannegowda RB, Agrawal A, Hemrajani D, Jain R, Mathur T. ‘Hot cross bun’ sign in a case of cerebrotendinous xanthomatosis: a rare neuroimaging observation. BMJ Case Rep 2013;2013:bcr2012006641.ArticlePubMedPMC
- 7. Kamm C, Healy DG, Quinn NP, Wüllner U, Moller JC, Schols L, et al. The fragile X tremor ataxia syndrome in the differential diagnosis of multiple system atrophy: data from the EMSA Study Group. Brain 2005;128(Pt 8):1855–1860.ArticlePubMedPDF
- 8. Gilman S, Wenning GK, Low PA, Brooks DJ, Mathias CJ, Trojanowski JQ, et al. Second consensus statement on the diagnosis of multiple system atrophy. Neurology 2008;71:670–676.ArticlePubMedPMC
- 9. Kasahara S, Miki Y, Kanagaki M, Kondo T, Yamamoto A, Morimoto E, et al. “Hot cross bun” sign in multiple system atrophy with predominant cerebellar ataxia: a comparison between proton density-weighted imaging and T2-weighted imaging. Eur J Radiol 2012;81:2848–2852.ArticlePubMed
- 10. Loh KB, Rahmat K, Lim SY, Ramli N. A Hot Cross Bun sign from diffusion tensor imaging and tractography perspective. Neurol India 2011;59:266–269.ArticlePubMed
REFERENCES
Figure & Data
References
Citations
- Progressive supranuclear palsy: A case report and brief review of the literature
Vivek Batheja, Morgan Fish, Aneri B. Balar, Jeffery P. Hogg, Dhairya A. Lakhani, Musharaf Khan
Radiology Case Reports.2024; 19(1): 250. CrossRef - A case of bilateral middle cerebellar peduncle infarction with hot cross bun sign
Daisuke Kuzume, Yuko Morimoto, Satoshi Tsutsumi, Masahiro Yamasaki, Naohisa Hosomi
Rinsho Shinkeigaku.2024; 64(3): 190. CrossRef - Immune‐mediated spastic ataxia masquerading as clinically probable multisystem atrophy in an elderly woman
Rithvik Ramesh, Anuhya Chadalawada, Pedapati Radhakrishna, Lakshmi Narasimhan Ranganathan, Philo Hazeena, Sundar Shanmugam, Deepa Avadhani
Clinical and Experimental Neuroimmunology.2024;[Epub] CrossRef - Food for Thought: A Review of Neuroradiographic Signs Inspired by Food
C.T. Zoppo, T. Taros, J. Singh, A.S. Puri, A.L. Kuhn
Neurographics.2024; 14(1): 29. CrossRef - Structural and Molecular Imaging for Clinically Uncertain Parkinsonism
Sanskriti Sasikumar, Antonio P. Strafella
Seminars in Neurology.2023; 43(01): 095. CrossRef - Anti‐kelchlike protein 11 antibody‐associated encephalitis: Two case reports and review of the literature
Alejandro León Betancourt, Anina Schwarzwald, Alban Millonig, Michael Oberholzer, Lidia Sabater, Helly Hammer, Nicole Kamber, Lara Diem, Andrew Chan, Robert Hoepner, Anke Salmen, Christoph Friedli
European Journal of Neurology.2023; 30(6): 1801. CrossRef - Hjerne med kors
Linh Tran, Tuba Ahmad, Anniken Haslund, Phuoc Ngoc Thi Nguyen
Tidsskrift for Den norske legeforening.2023;[Epub] CrossRef - Atypical findings: Atypical parkinsonian syndromes or Atypical parkinsonian syndromes look-alikes
Fatma Zehra Calikusu, Sema Akkus, Esra Kochan Kizilkilic, Burc Cagri Poyraz, Ali Tarik Altunç, Gunes Kiziltan, Aysegul Gunduz
Clinical Neurology and Neurosurgery.2023; 233: 107975. CrossRef - Spinocerebellar ataxia-type 34: A case report and brief review of the literature
Vivek Batheja, Morgan Fish, Aneri B. Balar, Siddhi Hedge, Jeffery P. Hogg, Dhairya A. Lakhani, Musharaf Khan
Radiology Case Reports.2023; 18(11): 3954. CrossRef - Mapping cortical disease-burden at individual-level in frontotemporal dementia: implications for clinical care and pharmacological trials
Mary Clare McKenna, Marlene Tahedl, Jasmin Lope, Rangariroyashe H. Chipika, Stacey Li Hi Shing, Mark A. Doherty, Jennifer C. Hengeveld, Alice Vajda, Russell L. McLaughlin, Orla Hardiman, Siobhan Hutchinson, Peter Bede
Brain Imaging and Behavior.2022; 16(3): 1196. CrossRef - The “Black Straight-Line Sign” in the Putamen in Diffusion-Weighted Imaging: A Potential Diagnostic MRI Marker for Multiple System Atrophy
Yiming Zheng, Xiwen Wang, Huajian Zhao, Yanyan Jiang, Ying Zhu, Jing Chen, Wei Sun, Zhaoxia Wang, Yunchuang Sun
Frontiers in Neurology.2022;[Epub] CrossRef - Radiological hints for differentiation of cerebellar multiple system atrophy from spinocerebellar ataxia
Hung-Chieh Chen, Li-Hua Lee, Jiing-Feng Lirng, Bing-wen Soong
Scientific Reports.2022;[Epub] CrossRef - The “Hot Cross Bun Sign” in Spinocerebellar Ataxia Types 2 and 7–Case Reports and Review of Literature
Ansuya Kasavelu Naidoo, Cait‐Lynn Deanne Wells, Yashvir Rugbeer, Neil Naidoo
Movement Disorders Clinical Practice.2022; 9(8): 1105. CrossRef - Magnetic resonance imaging abnormalities as a marker of multiple system atrophy in isolated rapid eye movement sleep behavior disorder
Amaia Muñoz-Lopetegi, Joan Berenguer, Alex Iranzo, Monica Serradell, Teresa Pujol, Carles Gaig, Esteban Muñoz, Eduard Tolosa, Joan Santamaría
Sleep.2021;[Epub] CrossRef - Hot Cross Bun Sign: A Case Report of Multiple System Atrophy Presenting Predominantly as Respiratory Insufficiency
Margiben Tusharbhai Bhatt, R. Sunil
Indian Journal of Respiratory Care.2021; 10(1): 148. CrossRef - Descriptive neuroradiology: beyond the hummingbird
Inna Page, Frank Gaillard
Practical Neurology.2020; 20(6): 463. CrossRef - Various Diseases and Clinical Heterogeneity Are Associated With “Hot Cross Bun”
Shuzhen Zhu, Hualing Li, Bin Deng, Jialing Zheng, Zifeng Huang, Zihan Chang, Yanjun Huang, Zhibo Wen, Yanran Liang, Mengjue Yu, Ling-Ling Chan, Eng-King Tan, Qing Wang
Frontiers in Aging Neuroscience.2020;[Epub] CrossRef - Hot cross bun sign
M. Portet, M. Filyridou, D. C. Howlett
Journal of Neurology.2019; 266(10): 2573. CrossRef - Progressive Supranuclear Palsy, Corticobasal Degeneration, and Multiple System Atrophy
Paul Greene
CONTINUUM: Lifelong Learning in Neurology.2019; 25(4): 919. CrossRef - Differential value of brain magnetic resonance imaging in multiple system atrophy cerebellar phenotype and spinocerebellar ataxias
Minkyeong Kim, Jong Hyeon Ahn, Yoonsu Cho, Ji Sun Kim, Jinyoung Youn, Jin Whan Cho
Scientific Reports.2019;[Epub] CrossRef
Comments on this article
 PubReader
PubReader ePub Link
ePub Link Cite
Cite

